Aetna Vision Benefits Claim Form
Aetna Vision Benefits Claim Form - Complete the aetna vision claim form. Copy of the itemized bill/receipt (s) copy of the eob. Web find the aetna vision claim form you require. Include diagnosis, services rendered, date of services, provider name, address, npi number and. Web aetna may provide the employer named above with any benefit calculation used in payment of this claim for the purpose of reviewing the experience and operation of the. Concerned parties names, places of residence and. Web vision insurance plans contain exclusions and limitations. Web submitting your claims electronically is quick, convenient and easy. Click below to complete an electronic or2. Attach any requested documentation, such as.
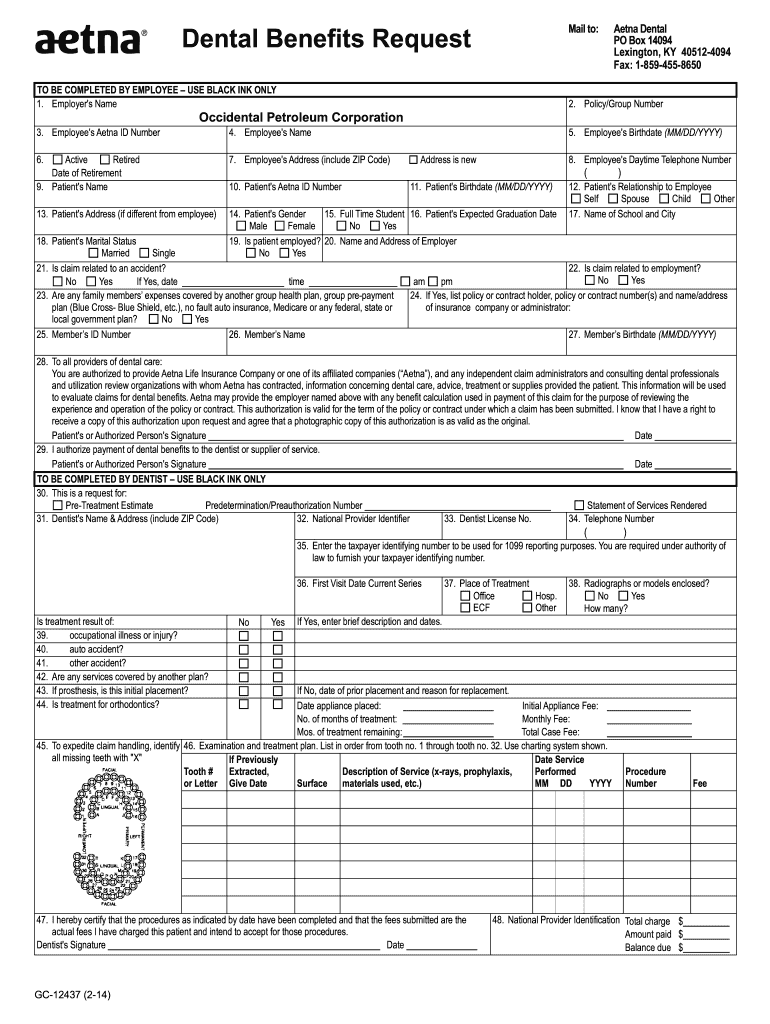
Attach any requested documentation, such as. Explore claims options tools that save you time and money eras,. Web vision benefits request refer to the back of your id card for claim mailing address to be completed by employee 1. Web vision insurance plans contain exclusions and limitations. Go green and get paid. Web to file a vision claim: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person submits an enrollm ent form for. Not all vision services are covered. Web we're sorry but vision benefits portal doesn't work properly without javascript enabled. Web submitting your claims electronically is quick, convenient and easy.
Web vision benefits request refer to the back of your id card for claim mailing address to be completed by employee 1. Web we're sorry but vision benefits portal doesn't work properly without javascript enabled. Include diagnosis, services rendered, date of services, provider name, address, npi number and. Web you can now submit your form online or by mail: Not all vision services are covered. Click below to complete an electronic or2. Complete the aetna vision claim form. Concerned parties names, places of residence and. Web a vision and hearing claim form can be found below for your convenience. Choose the option that works best for you.
Aetna Reimbursement Form Fill Out and Sign Printable PDF Template
Web aetna may provide the employer named above with any benefit calculation used in payment of this claim for the purpose of reviewing the experience and operation of the. Copy of the itemized bill/receipt (s) copy of the eob. Go green and getor paid faster.paperwork attached below. Choose the option that works best for you. Web find the aetna vision.

Aetna Medicare Advantage Plans Dental, Hearing & Vision Benefits
Web vision benefits request refer to the back of your id card for claim mailing address to be completed by employee 1. Web fill out this form if you paid a provider for covered medical, dental, vision, hearing or vaccination services and want to request reimbursement. Web complete and return theclaim form. Complete and return the claim form. Web health.
Downloads Carpenters Benefit Funds of Philadelphia
Go green and getor paid faster.paperwork attached below. Web a vision and hearing claim form can be found below for your convenience. Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person submits an enrollm ent form for. Web we're sorry but vision benefits portal doesn't work properly without javascript enabled. Not.

Aetna Medicare Advantage Plans for 2022
Go green and getor paid faster.paperwork attached below. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its. Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person submits an enrollm ent form for..
Understanding Medicare Advantage Dental Benefits Aetna
Go green and get paid. Web we're sorry but vision benefits portal doesn't work properly without javascript enabled. If you're filing a claim for more than one person, a separate form is needed for. Concerned parties names, places of residence and. Web this form can be used to submit a claim for medical, dental, vision, or pharmaceutical services.
Aetna Eylea Prior Authorization Form Fill Out and Sign Printable PDF
Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person submits an enrollm ent form for. Complete and return the claim form. Web a vision and hearing claim form can be found below for your convenience. Fill out this form if you’re asking for a medical, dental, vision, hearing, or vaccine reimbursement.
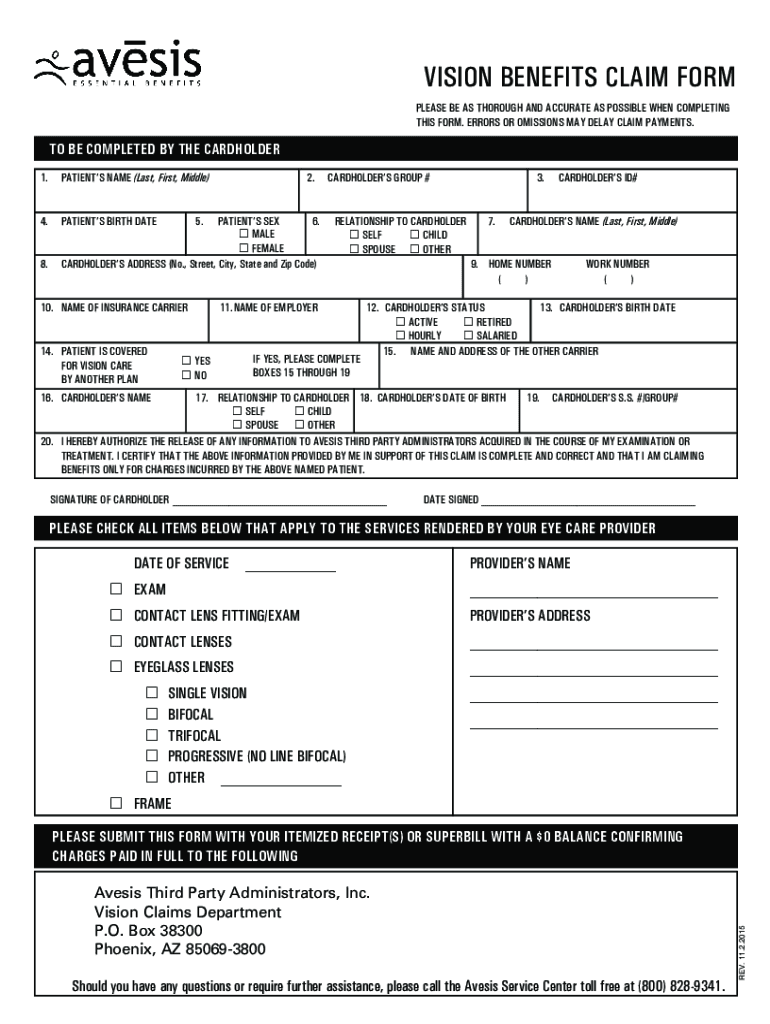
20152022 Avesis Vision Benefits Claim Form Fill Online, Printable
Web you can now submit your form online or by mail: See plan documents for a complete description of benefits, exclusions,. Not all vision services are covered. If you're filing a claim for more than one person, a separate form is needed for. Web aetna may provide the employer named above with any benefit calculation used in payment of this.
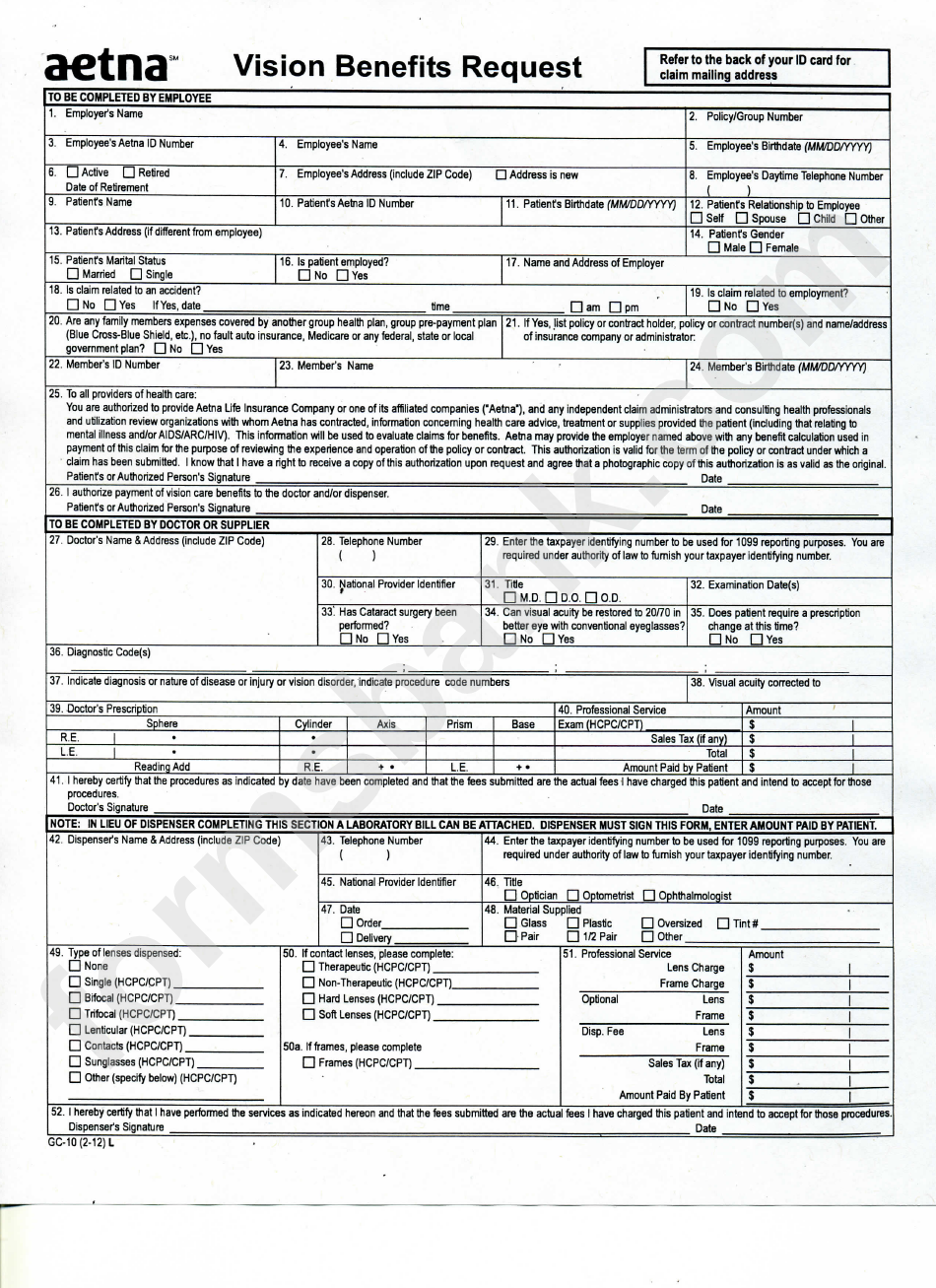
Form Gc10 (212) Vision Benefits Medical Claim Form And Medical
Web to file a vision claim: For complete terms and conditions, review the claim form. Include diagnosis, services rendered, date of services, provider name, address, npi number and. Web aetna may provide the employer named above with any benefit calculation used in payment of this claim for the purpose of reviewing the experience and operation of the. Please enable it.
Aetna Better Health Of Kansas Login Aetna Better Health Pa Picshealth
Web this form can be used to submit a claim for medical, dental, vision, or pharmaceutical services. For complete terms and conditions, review the claim form. Click below to complete an electronic or2. Web fill out this form if you paid a provider for covered medical, dental, vision, hearing or vaccination services and want to request reimbursement. Web we're sorry.

Medical Claim form Template Beautiful Medical Claim Template Free
Please enable it to continue. If you're filing a claim for more than one person, a separate form is needed for. Web when to use this form? Complete the aetna vision claim form. Go green and get paid.
Attach Any Requested Documentation, Such As.
Include diagnosis, services rendered, date of services, provider name, address, npi number and. Web health insurance plans | aetna Web we're sorry but vision benefits portal doesn't work properly without javascript enabled. Concerned parties names, places of residence and.
If You're Filing A Claim For More Than One Person, A Separate Form Is Needed For.
Complete and return the claim form. Complete the aetna vision claim form. Copy of the itemized bill/receipt (s) copy of the eob. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its.
Web Aetna May Provide The Employer Named Above With Any Benefit Calculation Used In Payment Of This Claim For The Purpose Of Reviewing The Experience And Operation Of The.
Web this form can be used to submit a claim for medical, dental, vision, or pharmaceutical services. Go green and getor paid faster.paperwork attached below. Web find the aetna vision claim form you require. Web you can now submit your form online or by mail:
See Plan Documents For A Complete Description Of Benefits, Exclusions,.
Web vision benefits request refer to the back of your id card for claim mailing address to be completed by employee 1. Web complete and return theclaim form. Web a vision and hearing claim form can be found below for your convenience. Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person submits an enrollm ent form for.