Bcbs Out Of Network Claim Form
Bcbs Out Of Network Claim Form - You can use these claim forms to ask us for reimbursement. Our forms are organized by state. You can submit your claim either online or by mail.* submit your claim. Ebilling (automatic debit) international claim form. Select your state below to view forms for your area. Web please read before completing the form on the next page. Web if your provider does not file your claim for you, you can call our customer service department at the number on the back of your id card and ask for a claim form. For those that use the horizon blue app use the horizon blue app to submit your claims for reimbursement: Web enrollee claims submission an enrollee, instead of the provider, submits a claim to the issuer, requesting payment for services that have been received. Medical or vision claim form.
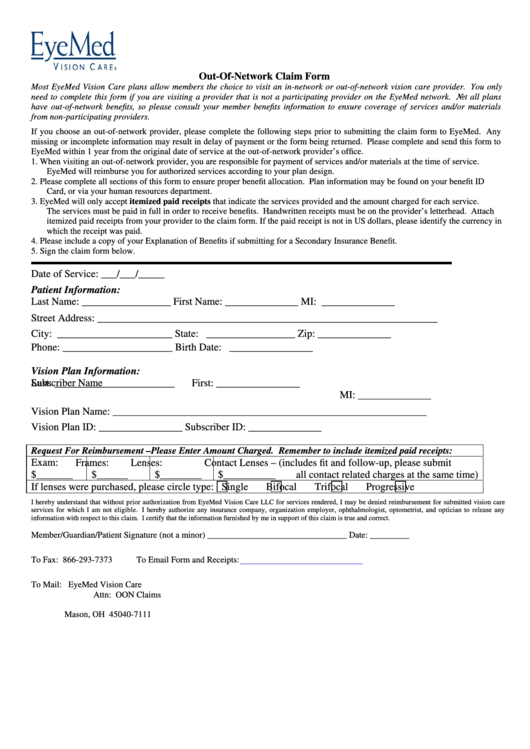
Medical or vision claim form. As a blue shield of california medicare advantage or medicare prescription drug plan member, you must. Web you can send a claim form to: Web please read before completing the form on the next page. Select your state below to view forms for your area. Web did you recently see a provider that was not in your plan’s network? Members can log in to view forms that are specific to their plan. If you do, then download the. Web if your provider does not file your claim for you, you can call our customer service department at the number on the back of your id card and ask for a claim form. Web find member claim forms, related forms such as claim forms for dental, national accounts and more.
• take a picture of your. As a blue shield of california medicare advantage or medicare prescription drug plan member, you must. Web did you recently see a provider that was not in your plan’s network? If you do, then download the. You can submit your claim either online or by mail.* submit your claim. (for care received out of network area) coordination of benefits. Select your state below to view forms for your area. This form is only needed to submit claims for services and supplies that are not submitted by your provider (i.e., out. To submit a claim electronically, please login and go to submit claims page. Web you can send a claim form to:

Bcbs Claim Review Form mekabdesigns
If you do, then download the. Ebilling (automatic debit) international claim form. Web enrollee claims submission an enrollee, instead of the provider, submits a claim to the issuer, requesting payment for services that have been received. You can submit your claim either online or by mail.* submit your claim. Web please read before completing the form on the next page.
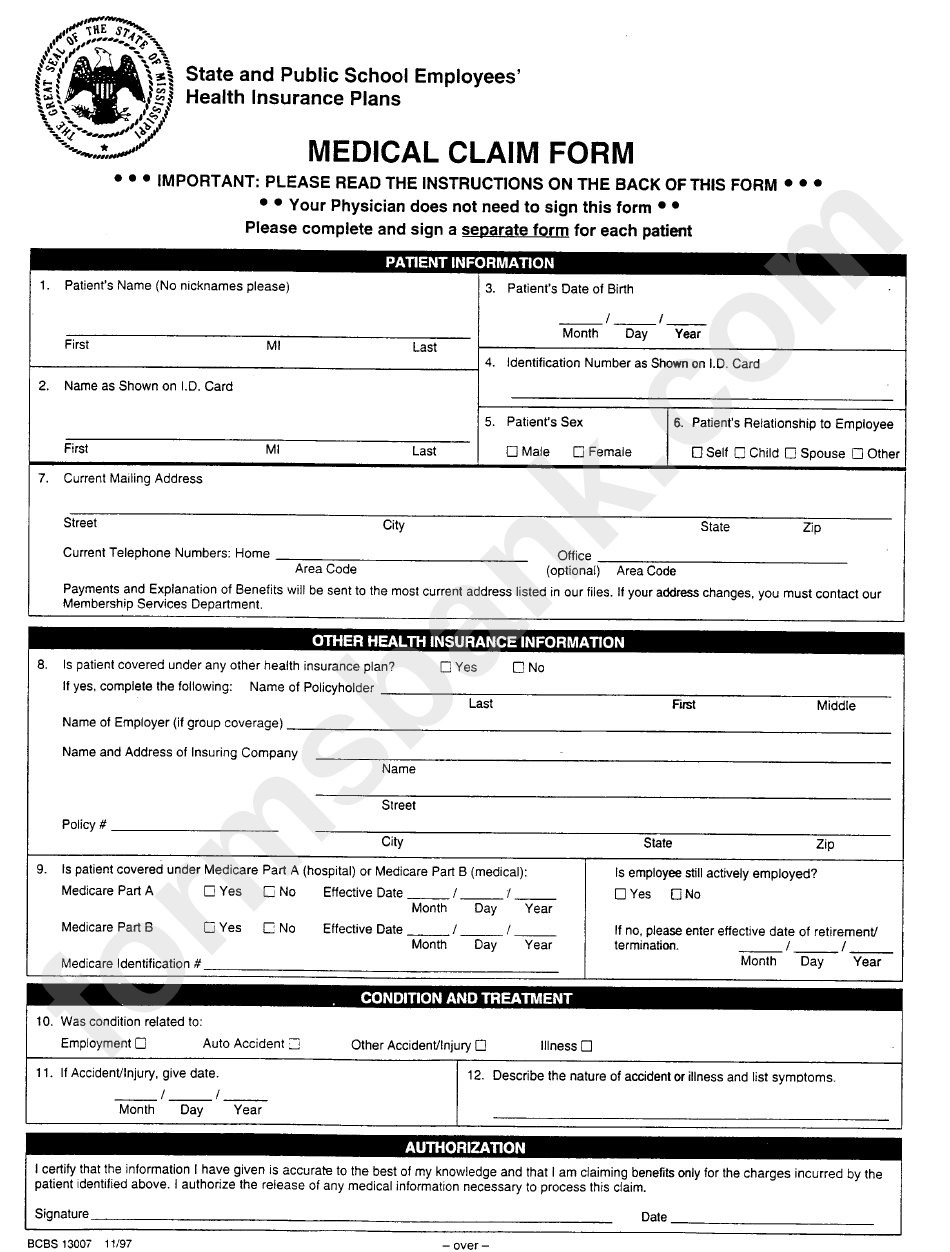
Form Bcbs 13007 State And Public School Employees Medical Claim Form
Ebilling (automatic debit) international claim form. Medical or vision claim form. As a blue shield of california medicare advantage or medicare prescription drug plan member, you must. Select your state below to view forms for your area. If you do, then download the.
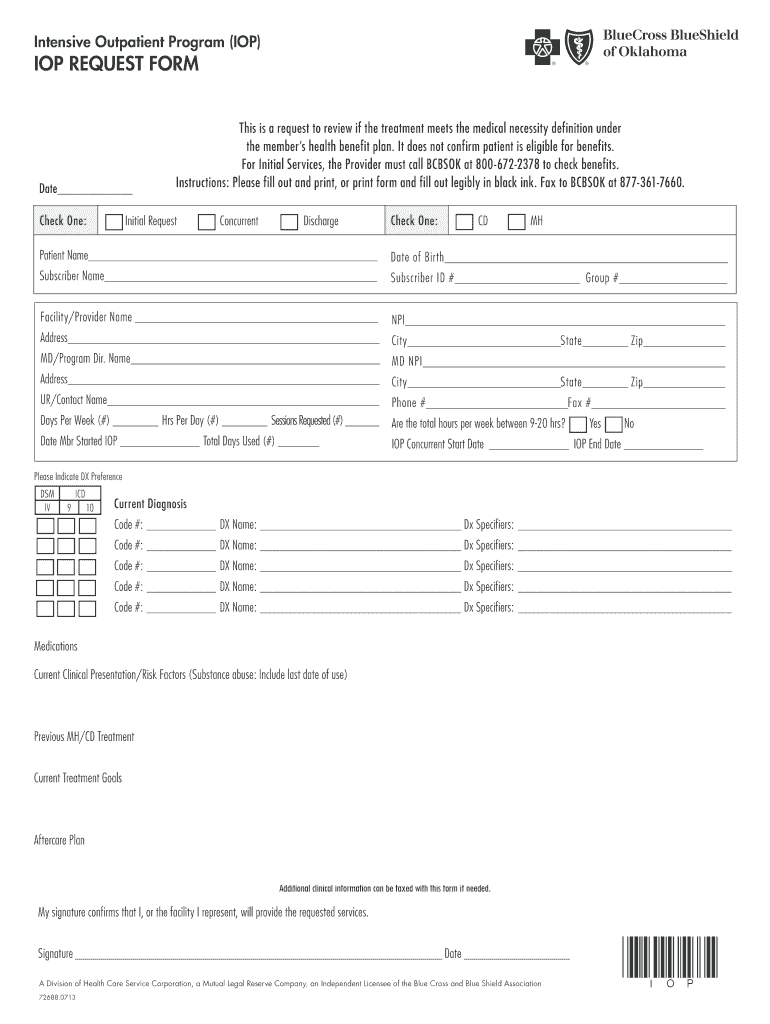
Bcbs Iop Request Form Fill Online, Printable, Fillable, Blank PDFfiller
You can use these claim forms to ask us for reimbursement. Select your state below to view forms for your area. You can submit your claim either online or by mail.* submit your claim. To submit a claim electronically, please login and go to submit claims page. • take a picture of your.
Bcbs Claim Review Form mekabdesigns
Web find member claim forms, related forms such as claim forms for dental, national accounts and more. Select your state below to view forms for your area. Web please read before completing the form on the next page. You can use these claim forms to ask us for reimbursement. As a blue shield of california medicare advantage or medicare prescription.
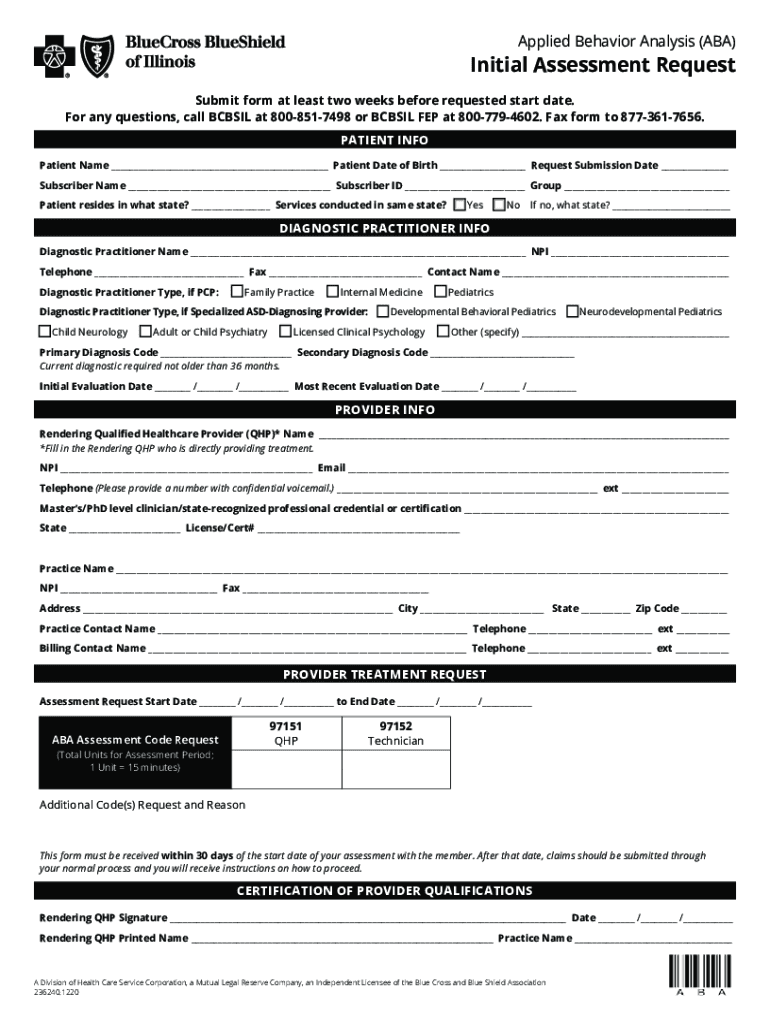
Form Aba Initial Fill Out and Sign Printable PDF Template signNow
Our forms are organized by state. Web you can send a claim form to: (for care received out of network area) coordination of benefits. You can use these claim forms to ask us for reimbursement. If you do, then download the.

Ms bcbs claim Fill out & sign online DocHub
This form is only needed to submit claims for services and supplies that are not submitted by your provider (i.e., out. • take a picture of your. You can use these claim forms to ask us for reimbursement. Ebilling (automatic debit) international claim form. Select your state below to view forms for your area.
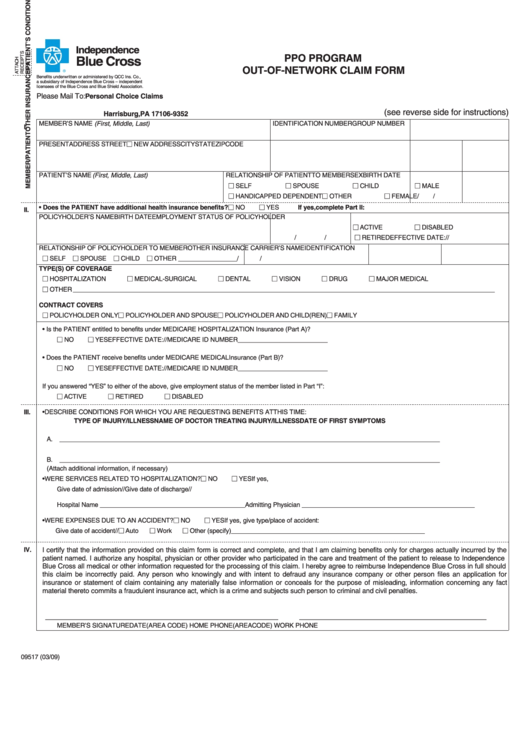
Ppo Program Claim Form Bcbs Pennsylvania printable pdf
(for care received out of network area) coordination of benefits. Our forms are organized by state. This form is only needed to submit claims for services and supplies that are not submitted by your provider (i.e., out. • take a picture of your. As a blue shield of california medicare advantage or medicare prescription drug plan member, you must.
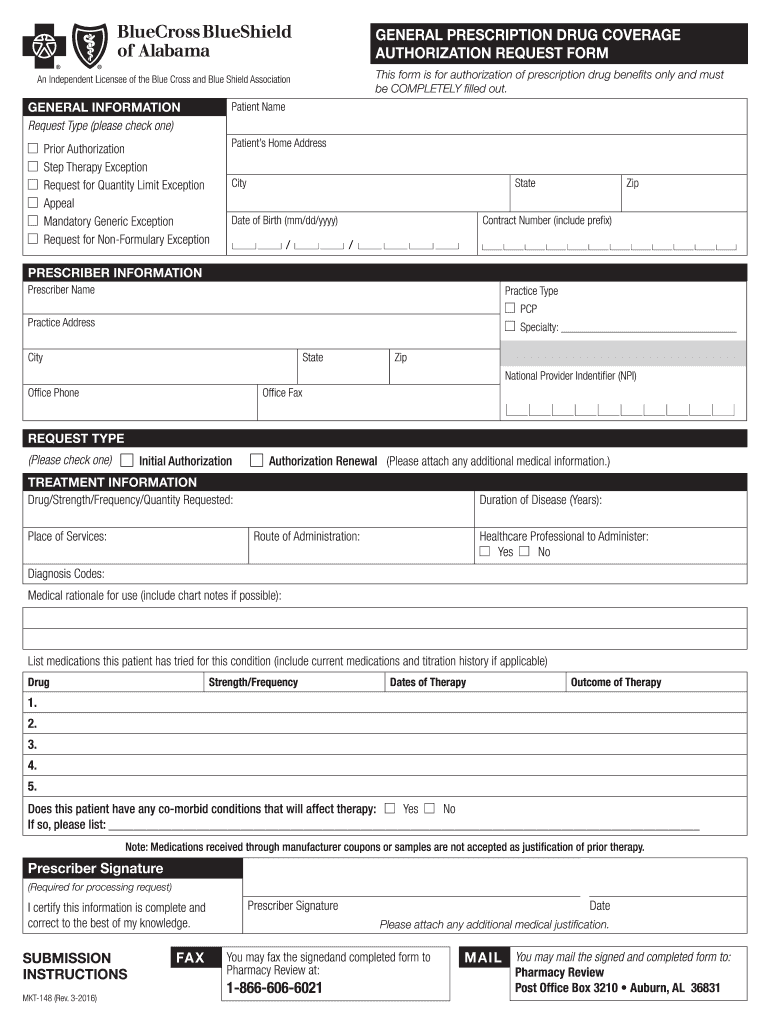
AL BCBS MKT148 2008 Fill and Sign Printable Template Online US
For those that use the horizon blue app use the horizon blue app to submit your claims for reimbursement: You can use these claim forms to ask us for reimbursement. Web find member claim forms, related forms such as claim forms for dental, national accounts and more. Web please read before completing the form on the next page. (for care.
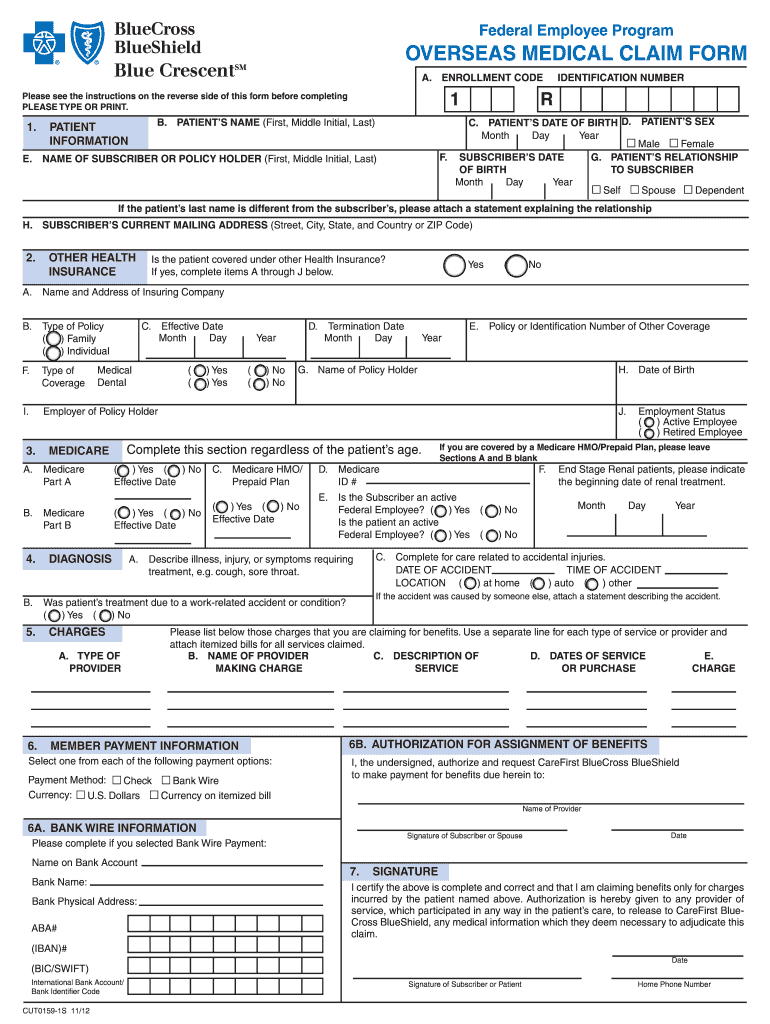
Federal Bcbs Basic Overseas Claim Form Fill Out and Sign Printable
Web please read before completing the form on the next page. Select your state below to view forms for your area. You can use these claim forms to ask us for reimbursement. Web find member claim forms, related forms such as claim forms for dental, national accounts and more. Web enrollee claims submission an enrollee, instead of the provider, submits.
Claim Form Date Of Service The Standard printable pdf
Web you can send a claim form to: Select your state below to view forms for your area. If you do, then download the. Ebilling (automatic debit) international claim form. Members can log in to view forms that are specific to their plan.
Members Can Log In To View Forms That Are Specific To Their Plan.
Medical or vision claim form. This form is only needed to submit claims for services and supplies that are not submitted by your provider (i.e., out. To submit a claim electronically, please login and go to submit claims page. For those that use the horizon blue app use the horizon blue app to submit your claims for reimbursement:
As A Blue Shield Of California Medicare Advantage Or Medicare Prescription Drug Plan Member, You Must.
Select your state below to view forms for your area. (for care received out of network area) coordination of benefits. Web if your provider does not file your claim for you, you can call our customer service department at the number on the back of your id card and ask for a claim form. You can use these claim forms to ask us for reimbursement.
Web Did You Recently See A Provider That Was Not In Your Plan’s Network?
Web enrollee claims submission an enrollee, instead of the provider, submits a claim to the issuer, requesting payment for services that have been received. Web please read before completing the form on the next page. Ebilling (automatic debit) international claim form. • take a picture of your.
Web Find Member Claim Forms, Related Forms Such As Claim Forms For Dental, National Accounts And More.
If you do, then download the. Web you can send a claim form to: You can submit your claim either online or by mail.* submit your claim. Our forms are organized by state.