Blue Cross Appeals Form
Blue Cross Appeals Form - If you have a problem with your blue cross blue shield of michigan service, you can use this form to file an appeal with us. You may file an appeal in writing by. Download an electronic copy of the blue cross nc member appeal. Your completed form or letter can. Web submit an appeal, send us a completed request for claim review form. Web filing a medical appeal. If you're a blue cross. • request a grievance if you have a complaint against blue cross or your. State health plan ppo ; Web to file a grievance, you may complete this form, or you may write a letter outlining as many details as possible regarding the incident in question.
State health plan ppo ; Download an electronic copy of the blue cross nc member appeal. Your completed form or letter can. Web po box 30055 appeal form. Web blue cross and blue shield of kansas (bcbsks) must receive your appeal within 180 days of the adverse decision. Mail or fax it to us using the address or fax number listed at the top of the form. Web provider appeal form please complete the following information and return this form with supporting documentation to the applicable address listed on the corresponding appeal. You can ask for an appeal if coverage or payment for an item or medical service is denied that you think should be covered. Web submit an appeal, send us a completed request for claim review form. This is due within one year of the date the claim was denied.
Web mail the completed form and appeal request to: This is due within one year of the date the claim was denied. You can submit up to two appeals for the. The appeal must be received by anthem blue cross (anthem) within 365. Call the bcbstx customer advocate department. If you are unable to. Web • request an appeal if you feel we didn’t cover or pay enough for a service or drug you received. Web fill out a health plan appeal request form. Web filing a medical appeal. You may file an appeal in writing by.

Wellcare Medicare Prior Authorization Forms
This is due within one year of the date the claim was denied. Web if there is a full or partial claim rejection or the payment is not the amount expected, submit a claims appeal. Print the complaint or appeal form (below) for your medicare health plan. If you are unable to. Complete the form and mail it to the.

Blue Cross Blue Shield Overseas Claim Form Fill Online, Printable
Web provider appeal form please complete the following information and return this form with supporting documentation to the applicable address listed on the corresponding appeal. If coverage or payment for an item or medical service is denied that you think should be covered. If you are unable to. The appeal must be received by anthem blue cross (anthem) within 365..
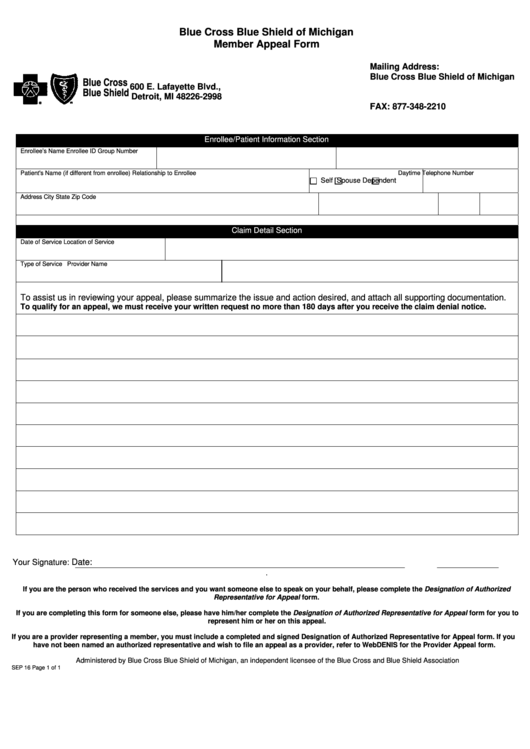
Fillable Blue Cross Blue Shield Of Michigan Member Appeal Form
If coverage or payment for an item or medical service is denied that you think should be covered. You can ask for an appeal: The appeal must be received by anthem blue cross (anthem) within 365. Web blue cross and blue shield of kansas (bcbsks) must receive your appeal within 180 days of the adverse decision. Web mail the completed.
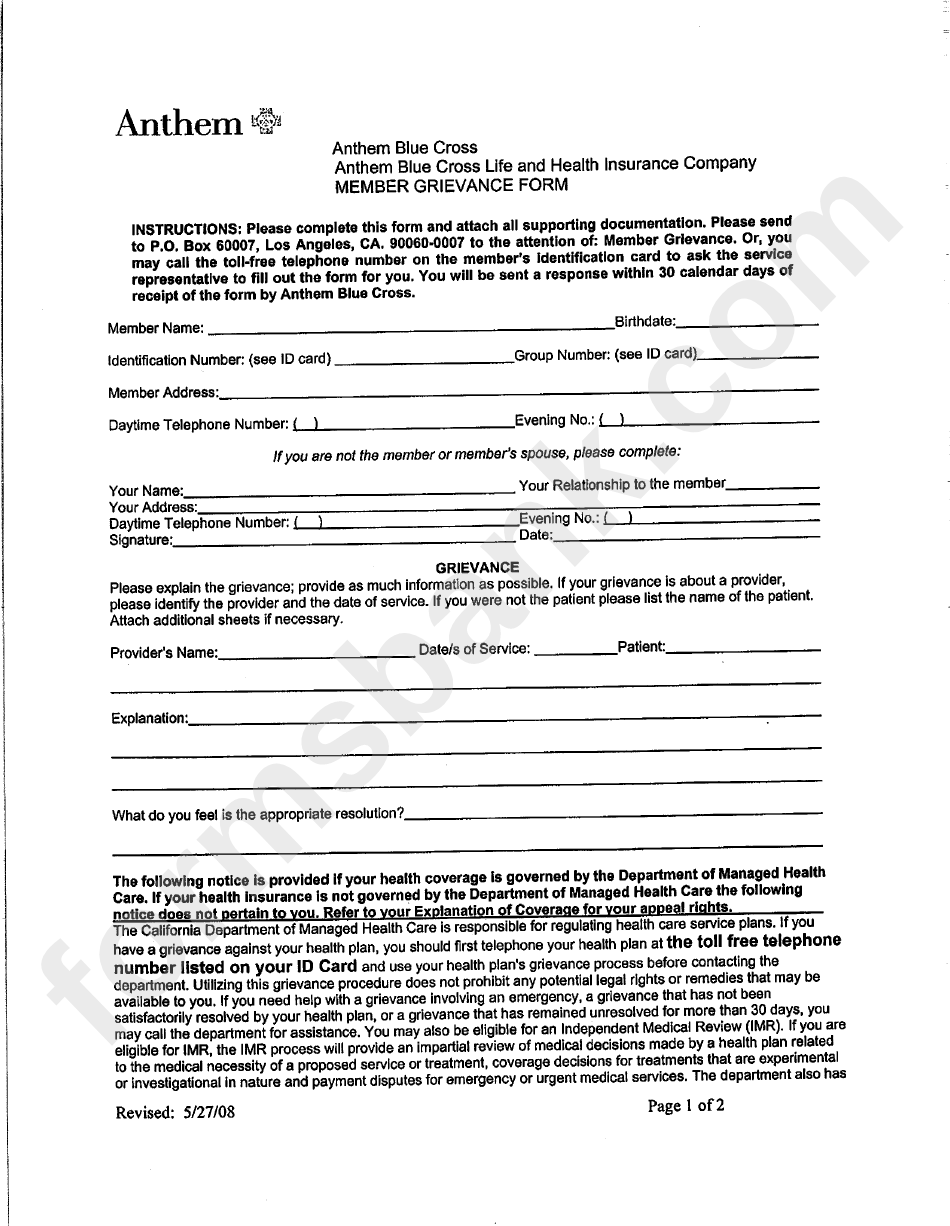
Anthem Blue Cross Member Grievance Form printable pdf download
If coverage or payment for an item or medical service is denied that you think should be covered. • request a grievance if you have a complaint against blue cross or your. The appeal must be received by anthem blue cross (anthem) within 365. Print the complaint or appeal form (below) for your medicare health plan. Web provider appeal form.
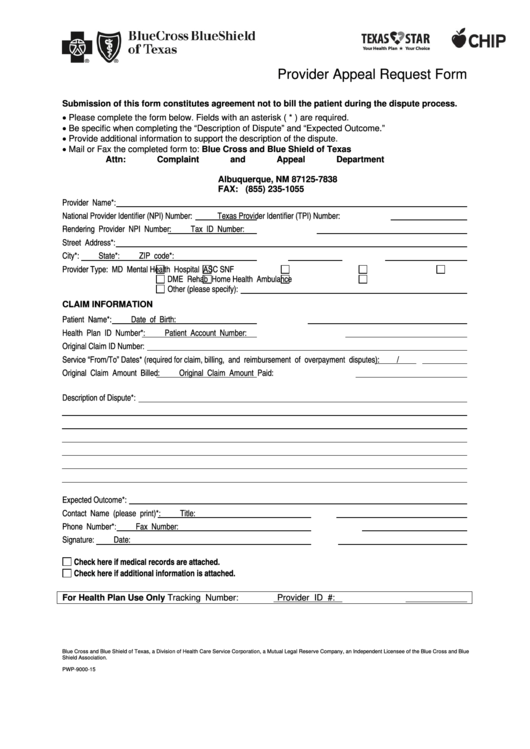
Bluecross Blueshield Of Texas Provider Appeal Request Form printable
Web blue cross and blue shield of kansas (bcbsks) must receive your appeal within 180 days of the adverse decision. Once the authorization is signed and dated, the provider will need to fax or mail the form and. You can ask for an appeal if coverage or payment for an item or medical service is denied that you think should.

Anthem Provider Dispute Resolution Form Colorado Fill Online
Your completed form or letter can. Web authorized representative) in order for a provider to appeal on their behalf. Web • request an appeal if you feel we didn’t cover or pay enough for a service or drug you received. You can submit up to two appeals for the. Web if there is a full or partial claim rejection or.
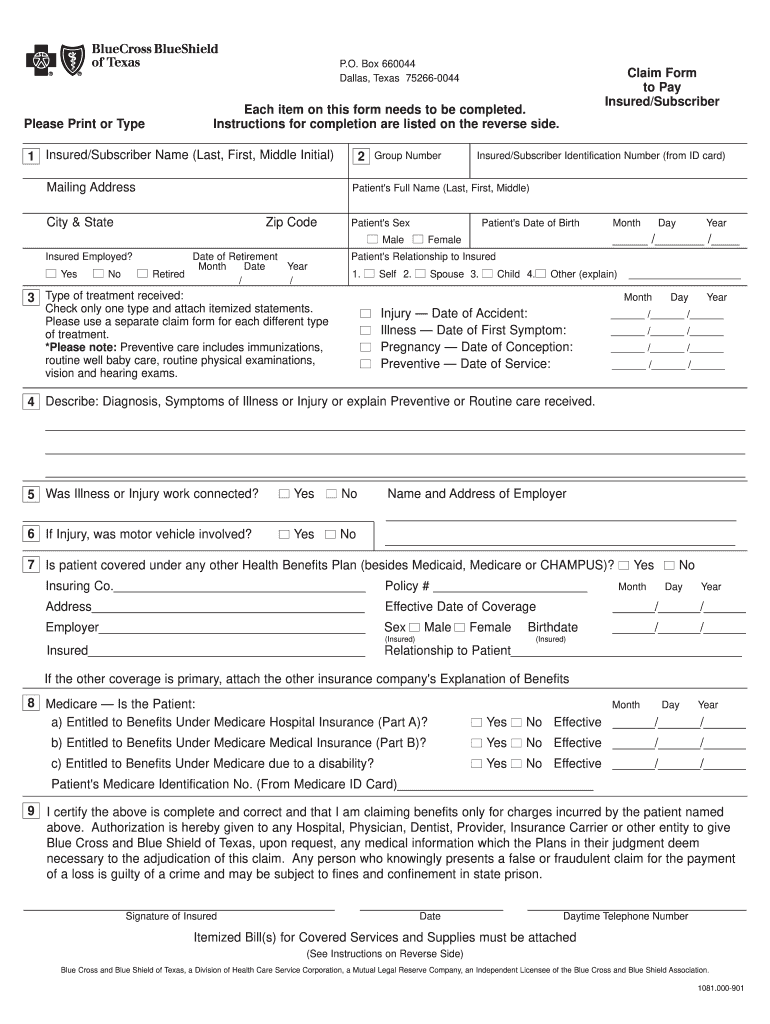
Bcbs Claim Form Fill Out and Sign Printable PDF Template signNow
If you have a problem with your blue cross blue shield of michigan service, you can use this form to file an appeal with us. Once the authorization is signed and dated, the provider will need to fax or mail the form and. Web to file a grievance, you may complete this form, or you may write a letter outlining.
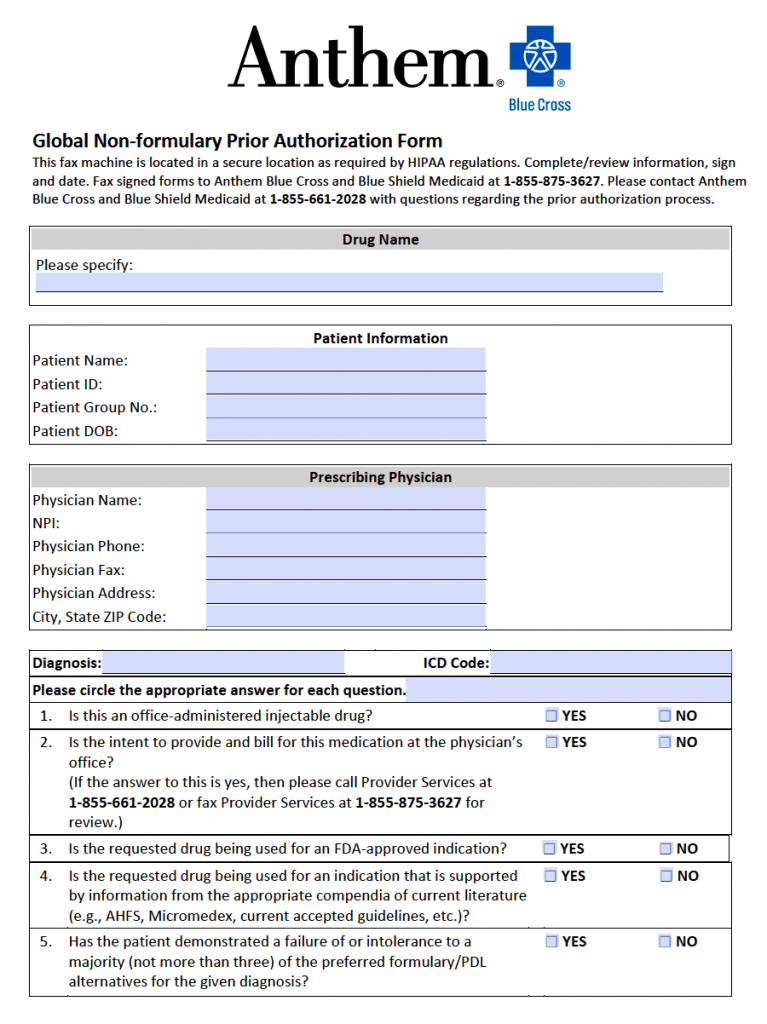
Free Anthem Blue Cross / Blue Shield Prior Prescription (Rx
The appeal must be received by anthem blue cross (anthem) within 365. Print the complaint or appeal form (below) for your medicare health plan. Bcbsks must make mail your appeal to: Web if there is a full or partial claim rejection or the payment is not the amount expected, submit a claims appeal. You can ask for an appeal:
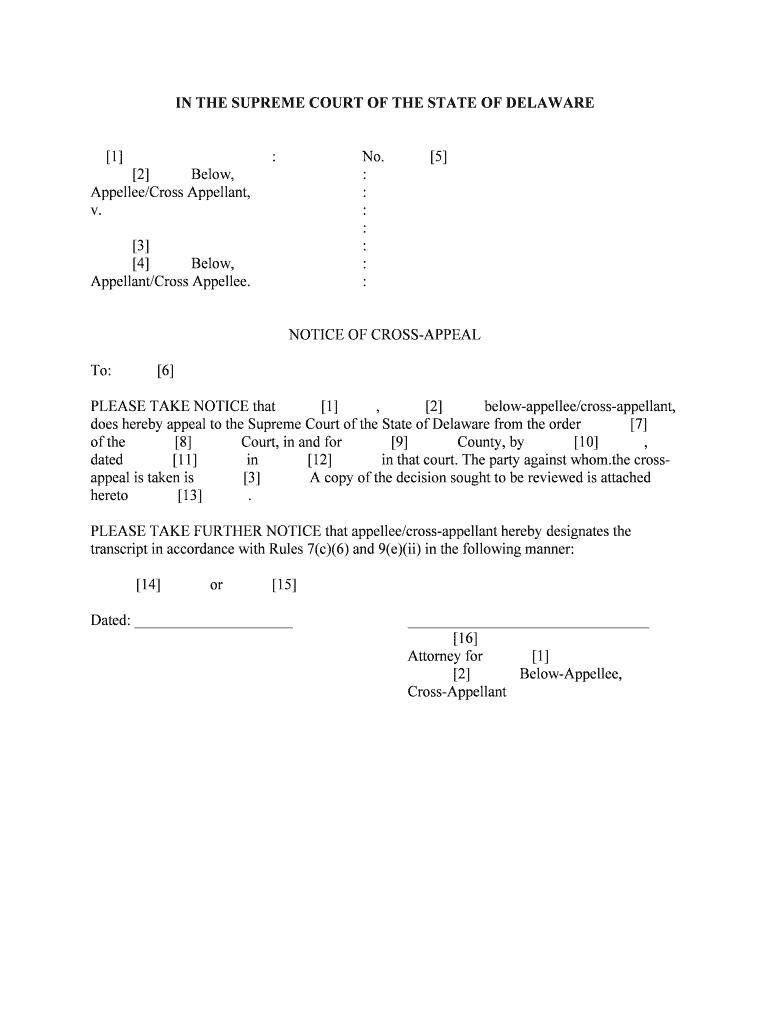
Rule 28 1 Cross Appeals Fourth Circuit Court of Appeals Form Fill Out
Web submit an appeal, send us a completed request for claim review form. You can submit up to two appeals for the. Web english authorized representative designation form use this form to select an individual or entity to act on your behalf during the disputed claims process. If you're a blue cross. Download an electronic copy of the blue cross.
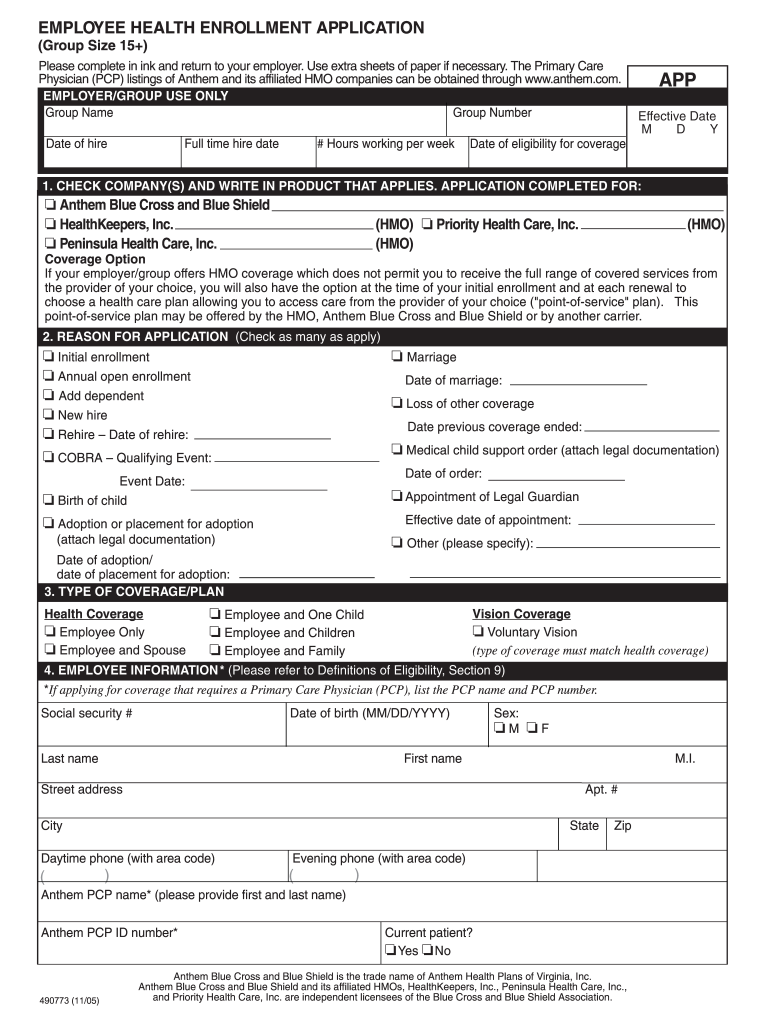
Anthem Enrollment Application Fill Out and Sign Printable PDF
If you have a problem with your blue cross blue shield of michigan service, you can use this form to file an appeal with us. Call the bcbstx customer advocate department. Print the complaint or appeal form (below) for your medicare health plan. You may file an appeal in writing by. Web fill out a health plan appeal request form.
By Mail Or By Fax:.
Web • request an appeal if you feel we didn’t cover or pay enough for a service or drug you received. You can ask for an appeal if coverage or payment for an item or medical service is denied that you think should be covered. The appeal must be received by anthem blue cross (anthem) within 365. You may file an appeal in writing by.
Download An Electronic Copy Of The Blue Cross Nc Member Appeal.
You can ask for an appeal: Call the bcbstx customer advocate department. Web appeal form who is this for? If you're a blue cross.
If You Are Unable To.
Web provider appeal form please complete the following information and return this form with supporting documentation to the applicable address listed on the corresponding appeal. State health plan ppo ; Web mail the completed form to: Web authorized representative) in order for a provider to appeal on their behalf.
Web Level I Provider Appeals For Billing/Coding Disputes And Medical Necessity Determinations Should Be Submitted By Sending A Written Request For Appeal Using The Level I Provider.
Web if there is a full or partial claim rejection or the payment is not the amount expected, submit a claims appeal. Web submit an appeal, send us a completed request for claim review form. Web mail the completed form and appeal request to: Web english authorized representative designation form use this form to select an individual or entity to act on your behalf during the disputed claims process.