Cms-1500 Claim Form Fields
Cms-1500 Claim Form Fields - Web cms 1500 dynamic list information. Web some services require that the actual number or quantity billed be clearly indicated on the claim form (e.g., multiple ostomy or urinary supplies). Fill out the health insurance claim form online and print it out for free. This form is the only version. Web the 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. When multiple items or services. It is the basic paper claim form prescribed by many payers for. Web field is constructed from qualifier and id number of first valid additional id of current insurer. The allowed qualifiers for box 33.b are: Most claims for these services and supplies may also be submitted through computer media claims.
The state of missouri does not require providers to use any particular form. Ad save time and spend less at filerx.com. Web some services require that the actual number or quantity billed be clearly indicated on the claim form (e.g., multiple ostomy or urinary supplies). Web select each field below for more information! Web field is constructed from qualifier and id number of first valid additional id of current insurer. Web 1500 required fields number and name. Download or email cms 1500 & more fillable forms, register and subscribe now! This form is the only version. Description and instructions n/a situational when submitting a medicare replacement plan claim, write or stamp “medicare replacement plan” in the left top. Most claims for these services and supplies may also be submitted through computer media claims.
Professionals and suppliers to transmit health care claims. The allowed qualifiers for box 33.b are: Web select each field below for more information! Most claims for these services and supplies may also be submitted through computer media claims. Web 1500 required fields number and name. Consisting of an alternate id or the subscriber's ssn. The state of missouri does not require providers to use any particular form. When multiple items or services. Web the 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Description and instructions n/a situational when submitting a medicare replacement plan claim, write or stamp “medicare replacement plan” in the left top.
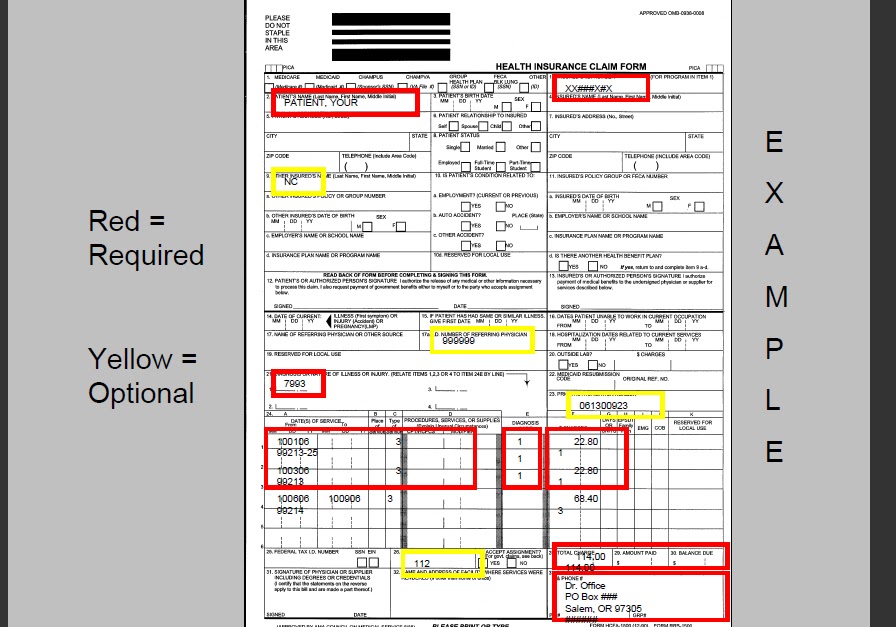
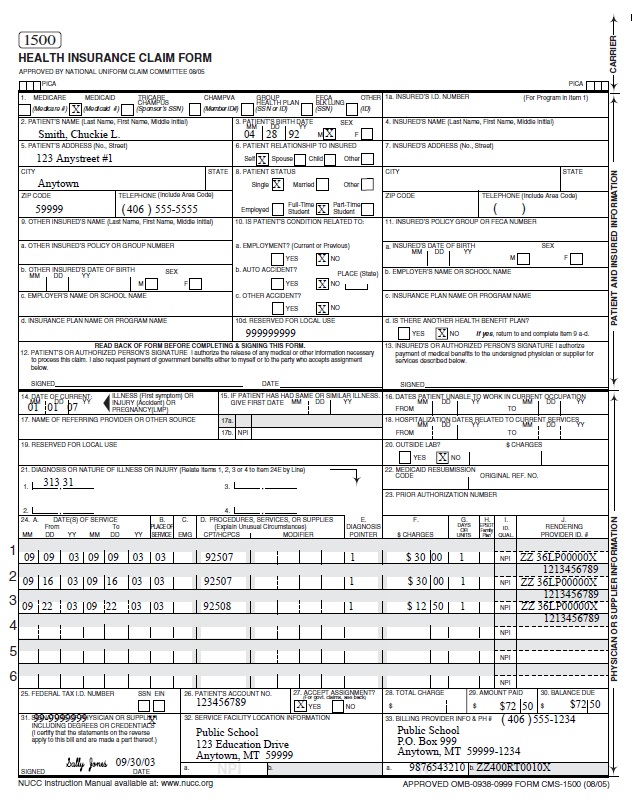
CMS 1500 full image with important field instruction CMS 1500 claim
Description and instructions n/a situational when submitting a medicare replacement plan claim, write or stamp “medicare replacement plan” in the left top. Web select each field below for more information! Web field is constructed from qualifier and id number of first valid additional id of current insurer. Web 1500 required fields number and name. The 837p (professional) is the standard.
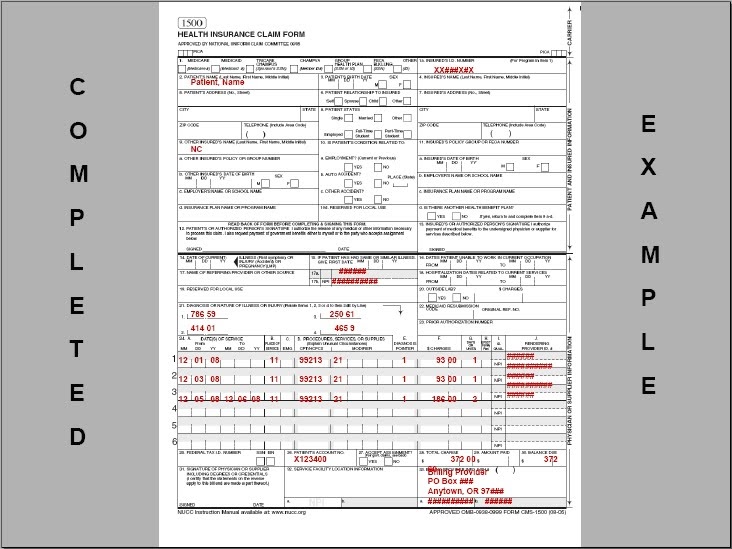
Completed CMS 1500 form CMS 1500 claim form and UB 04 form
Web select each field below for more information! Download or email cms 1500 & more fillable forms, register and subscribe now! This form is the only version. Web 1500 required fields number and name. Professionals and suppliers to transmit health care claims.
MD OnLine Resources CMS1500
Consisting of an alternate id or the subscriber's ssn. Download or email cms 1500 & more fillable forms, register and subscribe now! Ad save time and spend less at filerx.com. Most claims for these services and supplies may also be submitted through computer media claims. This form is the only version.

Cms 1500 Claim Form Fields Universal Network
Description and instructions n/a situational when submitting a medicare replacement plan claim, write or stamp “medicare replacement plan” in the left top. Most claims for these services and supplies may also be submitted through computer media claims. This form is the only version. The allowed qualifiers for box 33.b are: The state of missouri does not require providers to use.

Professional Claim (CMS1500) Field Descriptions
Web 1500 required fields number and name. Web cms 1500 dynamic list information. Professionals and suppliers to transmit health care claims. When multiple items or services. Web field is constructed from qualifier and id number of first valid additional id of current insurer.

Cms 1500 Claim Form Fields Universal Network
Fill out the health insurance claim form online and print it out for free. It is the basic paper claim form prescribed by many payers for. Download or email cms 1500 & more fillable forms, register and subscribe now! Web the 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Most claims for.
Insurance Claim Form Cms 1500 Cms 1500 Claim Form Tutorial Using And
Professionals and suppliers to transmit health care claims. The allowed qualifiers for box 33.b are: Web select each field below for more information! The state of missouri does not require providers to use any particular form. Ad save time and spend less at filerx.com.

1500 Claim Form Template SampleTemplatess SampleTemplatess
Web select each field below for more information! Web some services require that the actual number or quantity billed be clearly indicated on the claim form (e.g., multiple ostomy or urinary supplies). Description and instructions n/a situational when submitting a medicare replacement plan claim, write or stamp “medicare replacement plan” in the left top. Web cms 1500 dynamic list information..
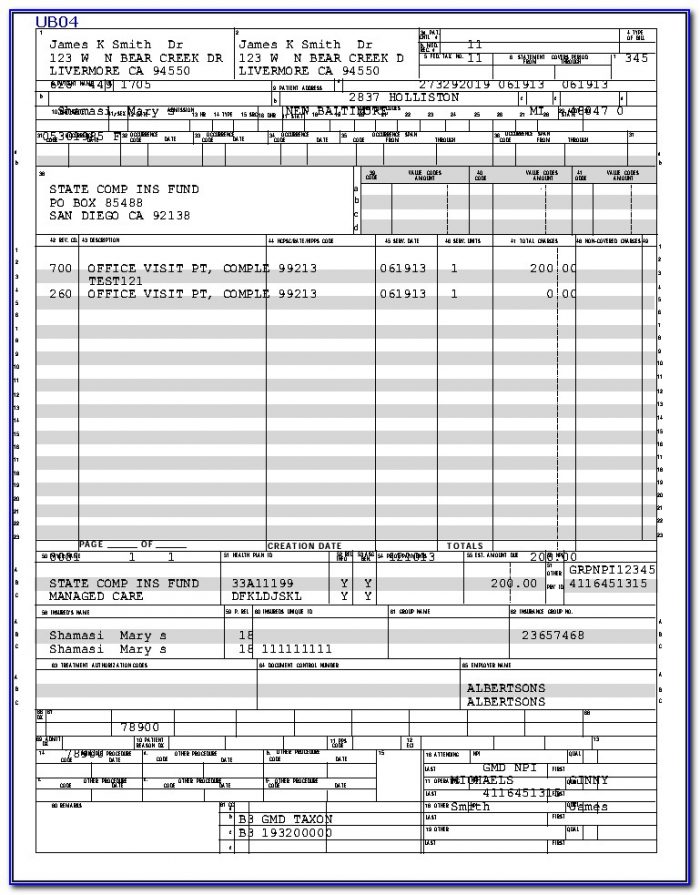
Ub 04 Form Printable Master of Documents
Most claims for these services and supplies may also be submitted through computer media claims. When multiple items or services. Web some services require that the actual number or quantity billed be clearly indicated on the claim form (e.g., multiple ostomy or urinary supplies). Fill out the health insurance claim form online and print it out for free. Web select.
schoolbasedservicesmanual
The 837p (professional) is the standard format used by health care. Web field is constructed from qualifier and id number of first valid additional id of current insurer. Most claims for these services and supplies may also be submitted through computer media claims. Ad save time and spend less at filerx.com. This form is the only version.
The Allowed Qualifiers For Box 33.B Are:
Description and instructions n/a situational when submitting a medicare replacement plan claim, write or stamp “medicare replacement plan” in the left top. Professionals and suppliers to transmit health care claims. Download or email cms 1500 & more fillable forms, register and subscribe now! Fill out the health insurance claim form online and print it out for free.
Ad Save Time And Spend Less At Filerx.com.
It is the basic paper claim form prescribed by many payers for. Consisting of an alternate id or the subscriber's ssn. The 837p (professional) is the standard format used by health care. Web some services require that the actual number or quantity billed be clearly indicated on the claim form (e.g., multiple ostomy or urinary supplies).
Web Select Each Field Below For More Information!
Web 1500 required fields number and name. The state of missouri does not require providers to use any particular form. Most claims for these services and supplies may also be submitted through computer media claims. When multiple items or services.
Web The 1500 Health Insurance Claim Form (1500 Claim Form) Answers The Needs Of Many Health Care Payers.
Web cms 1500 dynamic list information. Web field is constructed from qualifier and id number of first valid additional id of current insurer. This form is the only version.