Dental Registration And History Form
Dental Registration And History Form - Different forms are available for children and adults. Best practices learn to build better forms and leverage them for greater impact on your organization. Head to toe dental registration and history form. Web dental registration and history form (psd) 1. If you are completing this form for another person, what is your name and relationship to that person? Web health history form email: Take advantage of the fast search and advanced cloud editor to produce a. Work to be done i understand that i am having the following work done: The document is available in both english and spanish; Then read and sign the section at the bottom of form.
Web dental treatment consent form please read and initial the items checked below. Download the data file or print your copy. Different forms are available for children and adults. Whether you need to register new patients for your hospital, clinic, health center, or private practice, our free patient registration forms will streamline the registration and onboarding process by seamlessly gathering patient information. Web dental students graduating in 2023. Then read and sign the section at the bottom of form. Take advantage of the fast search and advanced cloud editor to produce a. Web what are your expectations and concerns regarding your dental treatment? Simple to fill out with individually numbered sections. Head to toe dental registration and history form.
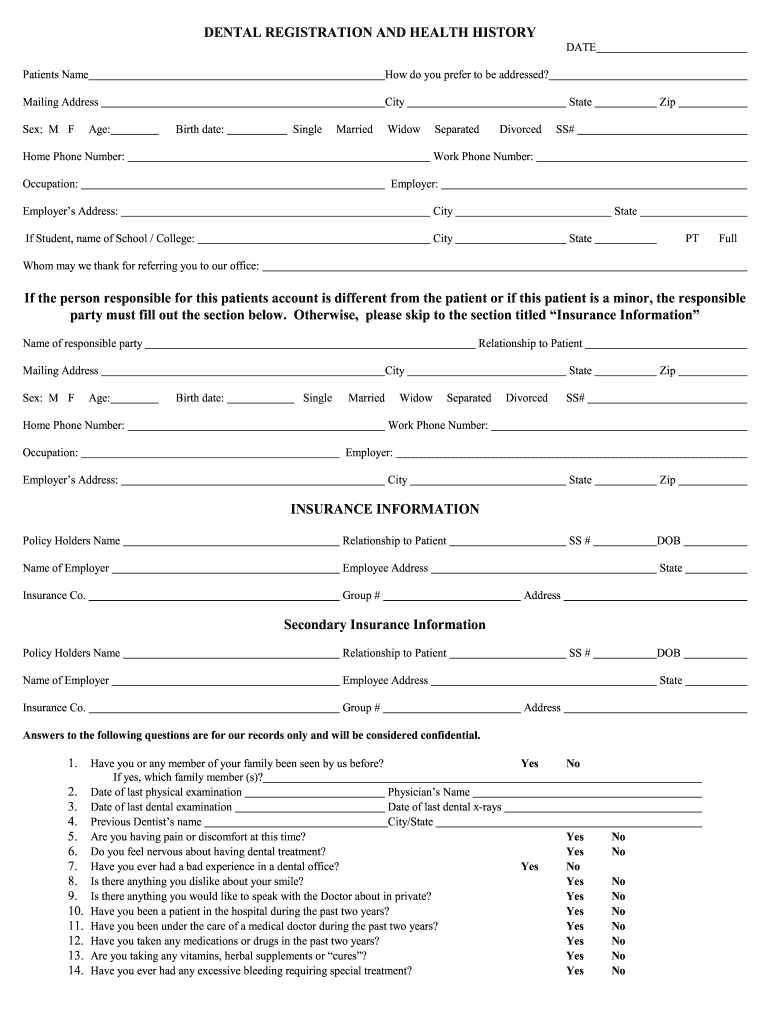
Web dental registration and history. If you are completing this form for another person, what is your name and relationship to that person? Your answers are for our records only and will be kept confidential subject to applicable laws. Web dental students graduating in 2023. Includes sections on patient information, insurance, history and more. Take advantage of the fast search and advanced cloud editor to produce a. Then read and sign the section at the bottom of form. Web dental registration and history form (psd) 1. Are you satisfied with the appearance of your teeth? Web exchange some of your registration and health information through a health information exchange between dental clinics at the medical center and the dental center to streamline the registration process for patients being seen at multiple locations (medical center, mission bay and dental center) and to provide treatment.

Registration and Dental History Forms Dental Record Forms
If you are completing this form for another person, what is your name and relationship to that person? The form is available in a digital, downloadable version or in print. Best practices learn to build better forms and leverage them for greater impact on your organization. Web exchange some of your registration and health information through a health information exchange.

Dental Patient Registration form Template Unique 27 Of Dental New
The sections required include the objective structured clinical exam (osce), endodontic. Includes sections on patient information, insurance, history and more. Fillings__ bridges__ crowns__ extractions__ impacted Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. 8.5 x 11 dental registration & history.
Dental Registration And History Form 20202021 Fill and Sign
Web dental registration and history form (psd) 1. Includes sections on patient information, insurance, history and more. Web landon state office building. Work to be done i understand that i am having the following work done: Fillings__ bridges__ crowns__ extractions__ impacted

Dental Medical History form Template New 27 Of Dental New Patient forms
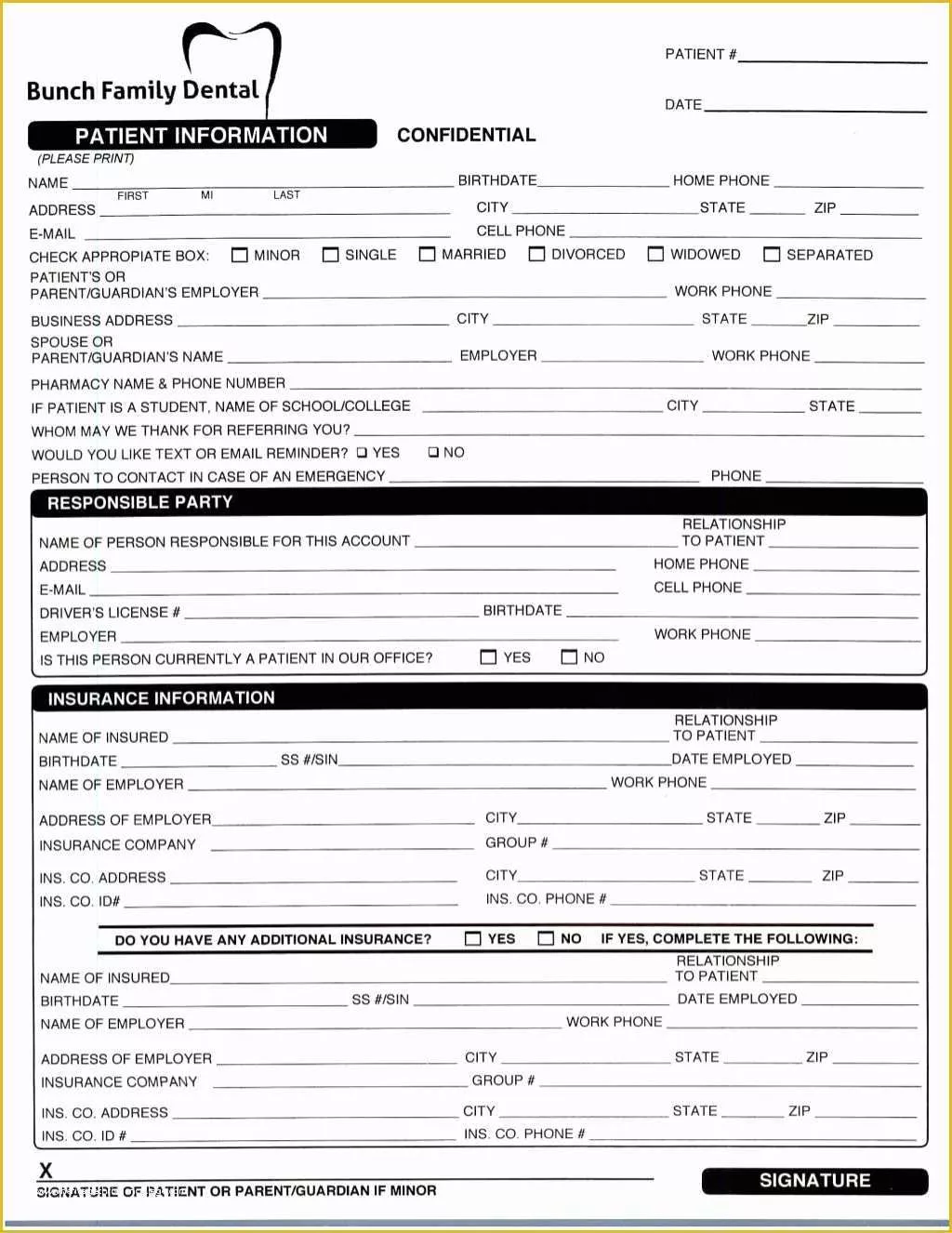
Web place your electronic signature to the pdf page. Fillings__ bridges__ crowns__ extractions__ impacted Whether you need to register new patients for your hospital, clinic, health center, or private practice, our free patient registration forms will streamline the registration and onboarding process by seamlessly gathering patient information. If not, what would you like to change Patient information i agree to.
Free Patient Registration form Template Of New Patient Registration
Web landon state office building. Then read and sign the section at the bottom of form. Best practices learn to build better forms and leverage them for greater impact on your organization. Web health history form email: Web dental students graduating in 2023.

Pin on My Blog
Web services are rendered and that health, dental and accident insurance policies are an arrangement between my insurance carrier and me. Fillings__ bridges__ crowns__ extractions__ impacted Patient information i agree to give perfect smiles dentistry 24 hours notice to cancel/reschedule my/my child's appointment * i agree patient name * first name last name birthday * mm/dd/yyyy ssn gender * male.
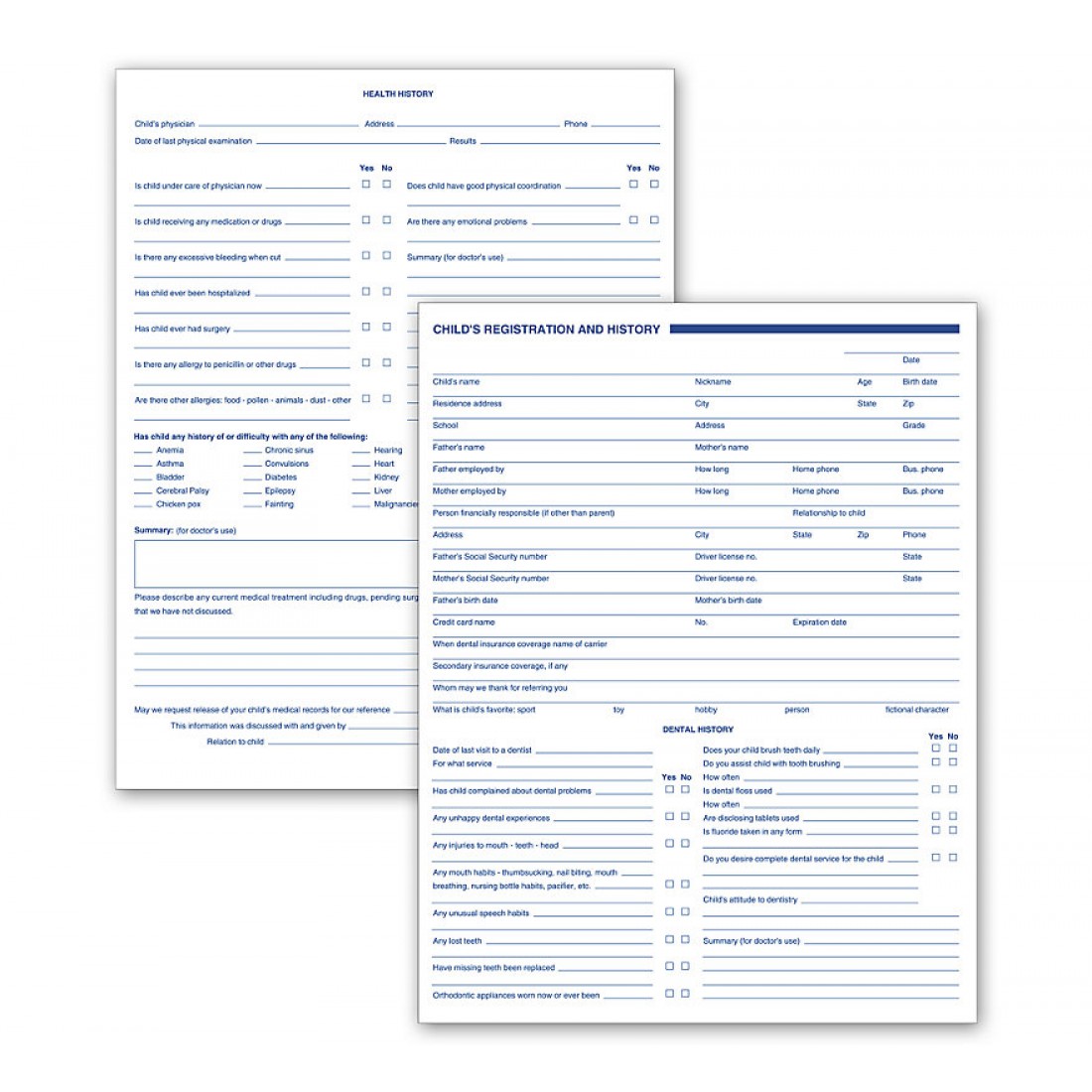
Dental Child Registration And History Forms 2 Sided
Your answers are for our records only and will be kept confidential subject to applicable laws. Web dental treatment consent form please read and initial the items checked below. Web what are your expectations and concerns regarding your dental treatment? Fillings__ bridges__ crowns__ extractions__ impacted Are you satisfied with the appearance of your teeth?
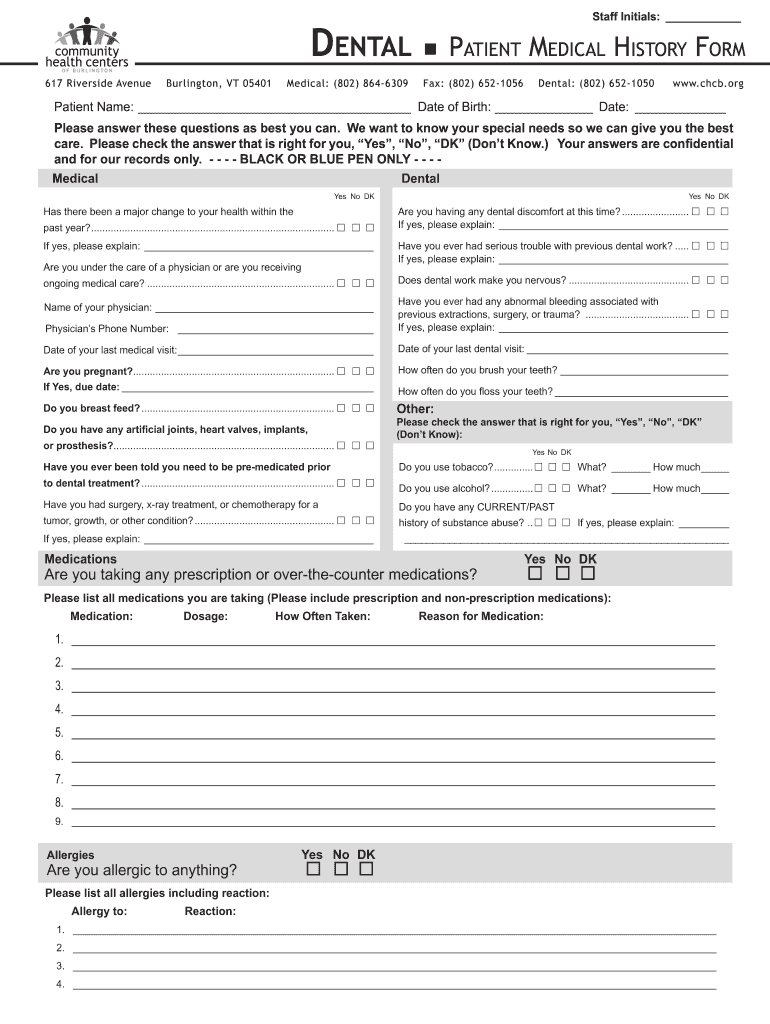
Dental Patient Medical Form Fill Online, Printable, Fillable, Blank
Web 4065 dental registration & history form. Web place your electronic signature to the pdf page. Take advantage of the fast search and advanced cloud editor to produce a. The form is available in a digital, downloadable version or in print. Web dental students graduating in 2023.

Patient Registration & History Form in Word and Pdf formats
Web landon state office building. Sections for contact information, prior cleanings, and medical history are included so you can collect all the information you need before a patient's first appointment. Web dental treatment consent form please read and initial the items checked below. Includes sections on patient information, insurance, history and more. Web place your electronic signature to the pdf.

Patient Registration & History Form in Word and Pdf formats page 4 of 6
Are you satisfied with the appearance of your teeth? Web landon state office building. Best practices learn to build better forms and leverage them for greater impact on your organization. Web dental registration and history form (psd) 1. Web services are rendered and that health, dental and accident insurance policies are an arrangement between my insurance carrier and me.
Best Practices Learn To Build Better Forms And Leverage Them For Greater Impact On Your Organization.
As required by law, our office adheres to written policies and procedures to protect the privacy of information about you that we create, receive or maintain. Web landon state office building. Web exchange some of your registration and health information through a health information exchange between dental clinics at the medical center and the dental center to streamline the registration process for patients being seen at multiple locations (medical center, mission bay and dental center) and to provide treatment. The sections required include the objective structured clinical exam (osce), endodontic.
Web Dental Registration And History.
If you are completing this form for another person, what is your name and relationship to that person? Web services are rendered and that health, dental and accident insurance policies are an arrangement between my insurance carrier and me. 8.5 x 11 dental registration & history form. Web dental students graduating in 2023.
Web What Are Your Expectations And Concerns Regarding Your Dental Treatment?
Simple to fill out with individually numbered sections. Fillings__ bridges__ crowns__ extractions__ impacted Sections for contact information, prior cleanings, and medical history are included so you can collect all the information you need before a patient's first appointment. Your answers are for our records only and will be kept confidential subject to applicable laws.
Web Patient Registration Forms Are Used To Register Patients For Procedures Offered At Medical Facilities.
If not, what would you like to change The form is available in a digital, downloadable version or in print. Web form allows you to gather complete information from patients. Patient information i agree to give perfect smiles dentistry 24 hours notice to cancel/reschedule my/my child's appointment * i agree patient name * first name last name birthday * mm/dd/yyyy ssn gender * male female other please upload a clear picture of the.