Form C-4
Form C-4 - Web use this form when a patient has reached maximum medical improvement and to render an opinion on permanent impairment, if any. Make sure that you review his entries before you leave the hospital. See instructions for schedule c (form 1040). Web date, sign, and list the facility you went to. (to report the first time you treated the patient,. Web form full name social security number (last) (first) (mi) home address (number and street) (city) (state) (zip code) as an employee of auburn university, my total compensation is. Number telephone doctor's signature degree. [noun] a high explosive composed of various chemicals that make it moldable and plastic. This committee has qualified as a multicandidate committee (see fec form 1m) 4. Web 1.this form is used for a workers' compensation, volunteer firefighters' or volunteer ambulance workers' benefit case as follows:
Web form full name social security number (last) (first) (mi) home address (number and street) (city) (state) (zip code) as an employee of auburn university, my total compensation is. 09 name of proprietor social security number (ssn) a principal business or profession,. Web 1.this form is used for a workers' compensation, volunteer firefighters' or volunteer ambulance workers' benefit case as follows: Web use this form to report continuing services. Web this form was mailed to the employer on: To confirm a telephone request for written. Make sure that you review his entries before you leave the hospital. To start the form, utilize the fill camp; When completing section 2, use information from the documentation the. Employer or authorized representative review and verification.
The physician fills out their part of the form, and sends a copy to your employer and the. When completing section 2, use information from the documentation the. Employer or authorized representative review and verification. This appendix contains ten sample notification forms. To start the form, utilize the fill camp; Web date, sign, and list the facility you went to. Bureau of consumer financial protection subject: Web use this form when a patient has reached maximum medical improvement and to render an opinion on permanent impairment, if any. Web use this form to report continuing services. See instructions for schedule c (form 1040).
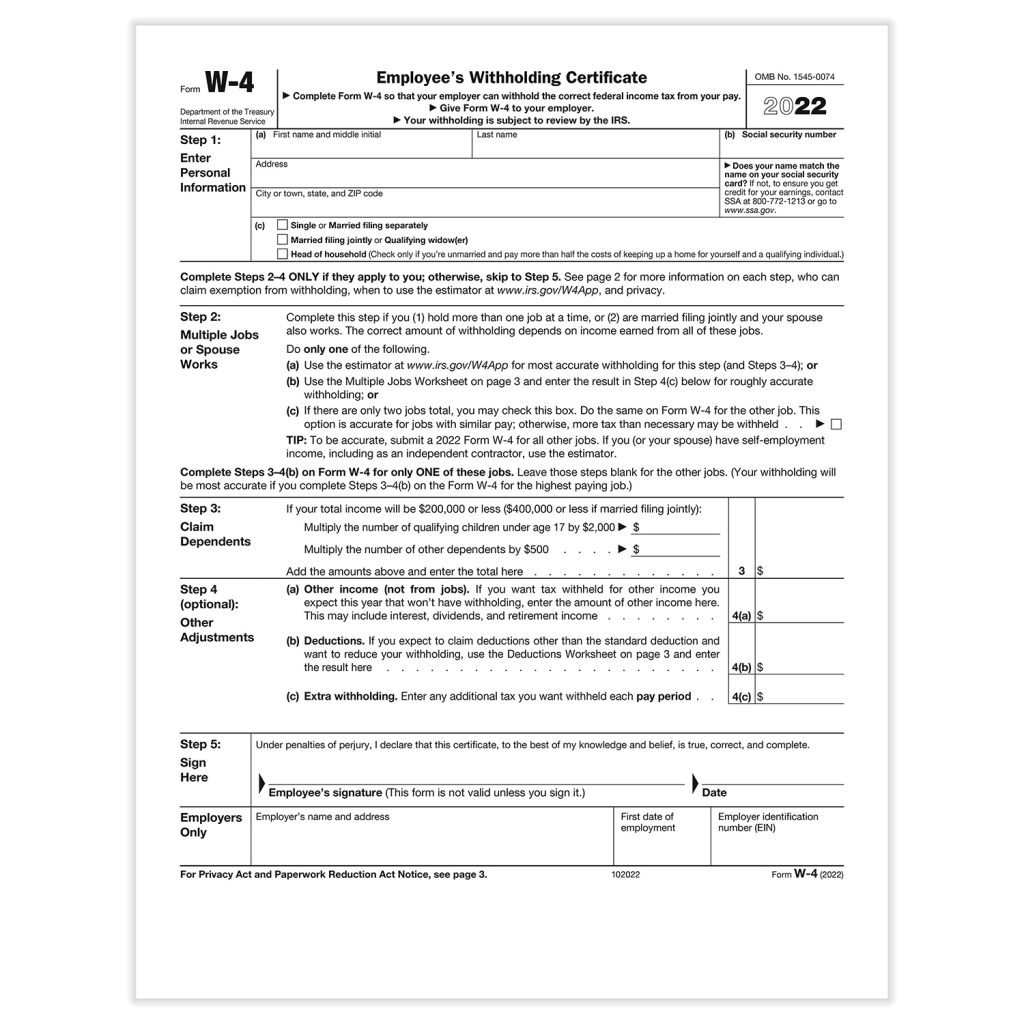
W2 Form 2022 Fillable Form 2023
Form 4720, return of certain excise taxes on charities and other persons. To start the form, utilize the fill camp; See instructions for schedule c (form 1040). [noun] a high explosive composed of various chemicals that make it moldable and plastic. This committee has qualified as a multicandidate committee (see fec form 1m) 4.
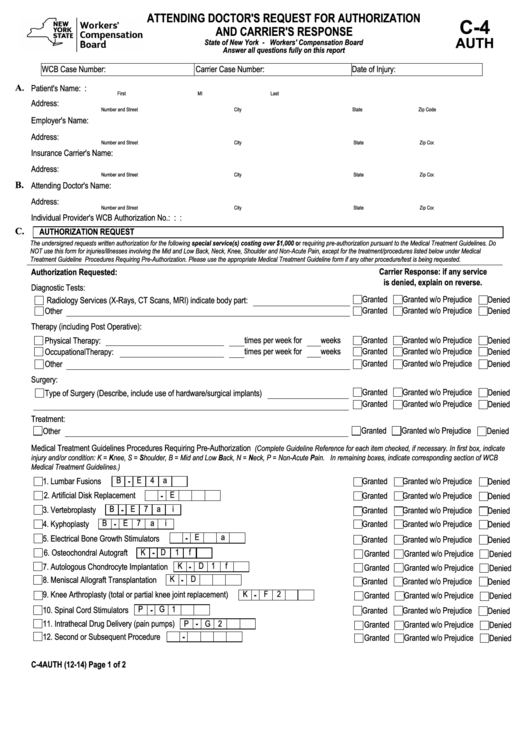
Fillable C4 Auth Workers' Compensation Board printable pdf download
When completing section 2, use information from the documentation the. Web use this form to report continuing services. Web 1.this form is used for a workers' compensation, volunteer firefighters' or volunteer ambulance workers' benefit case as follows: (to report the first time you treated the patient,. This form must be attached to and filed.
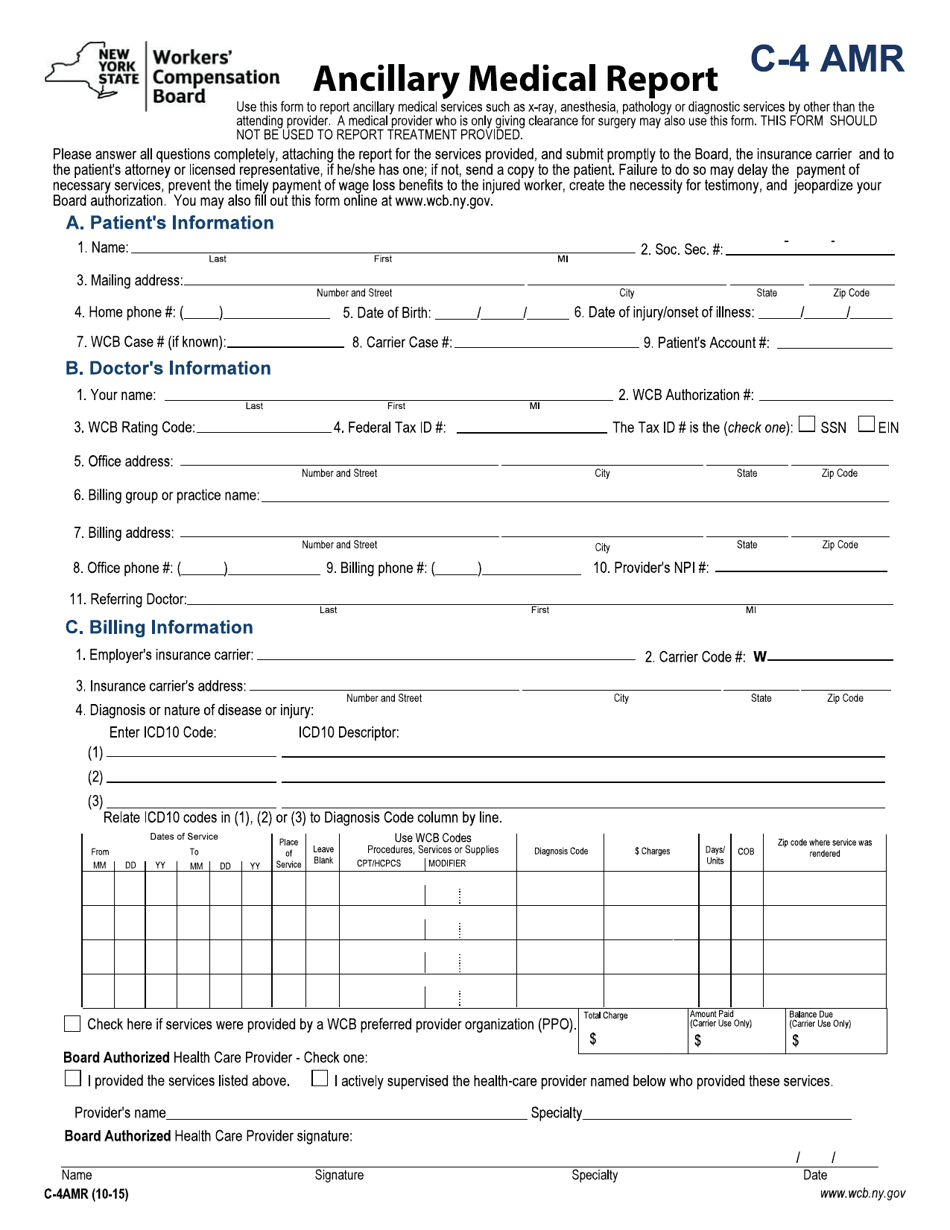
Form C4 AMR Download Fillable PDF or Fill Online Ancillary Medical
This committee has qualified as a multicandidate committee (see fec form 1m) 4. Web use this form when a patient has reached maximum medical improvement and to render an opinion on permanent impairment, if any. 09 name of proprietor social security number (ssn) a principal business or profession,. To start the form, utilize the fill camp; Bureau of consumer financial.
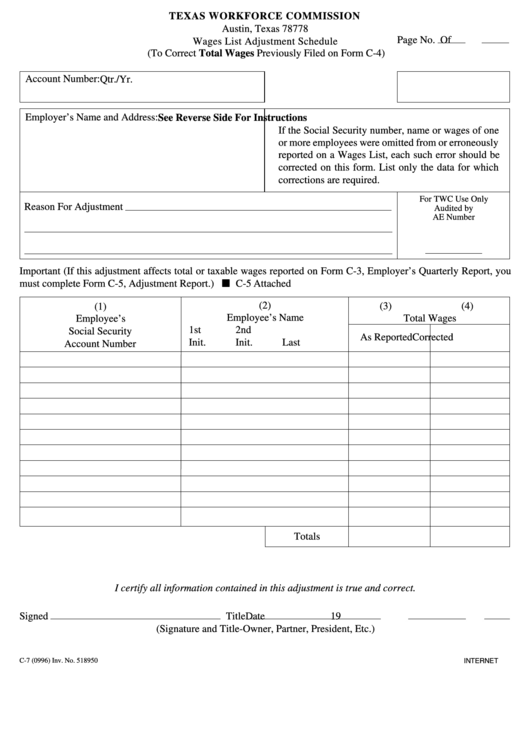
Form C7 Texas Workforce Commission printable pdf download
To start the form, utilize the fill camp; Web attach to form 1040 or 1041. Web use this form when a patient has reached maximum medical improvement and to render an opinion on permanent impairment, if any. This committee has qualified as a multicandidate committee (see fec form 1m) 4. Web 1.this form is used for a workers' compensation, volunteer.
/Title 4/Title 4 - Division 18 - Chapter 8 - Article 3 - Appendix C_4.png)
Appendix C State Regulations US Law LII / Legal Information
This form must be attached to and filed. Form 4720, return of certain excise taxes on charities and other persons. Number telephone doctor's signature degree. This appendix contains ten sample notification forms. [noun] a high explosive composed of various chemicals that make it moldable and plastic.
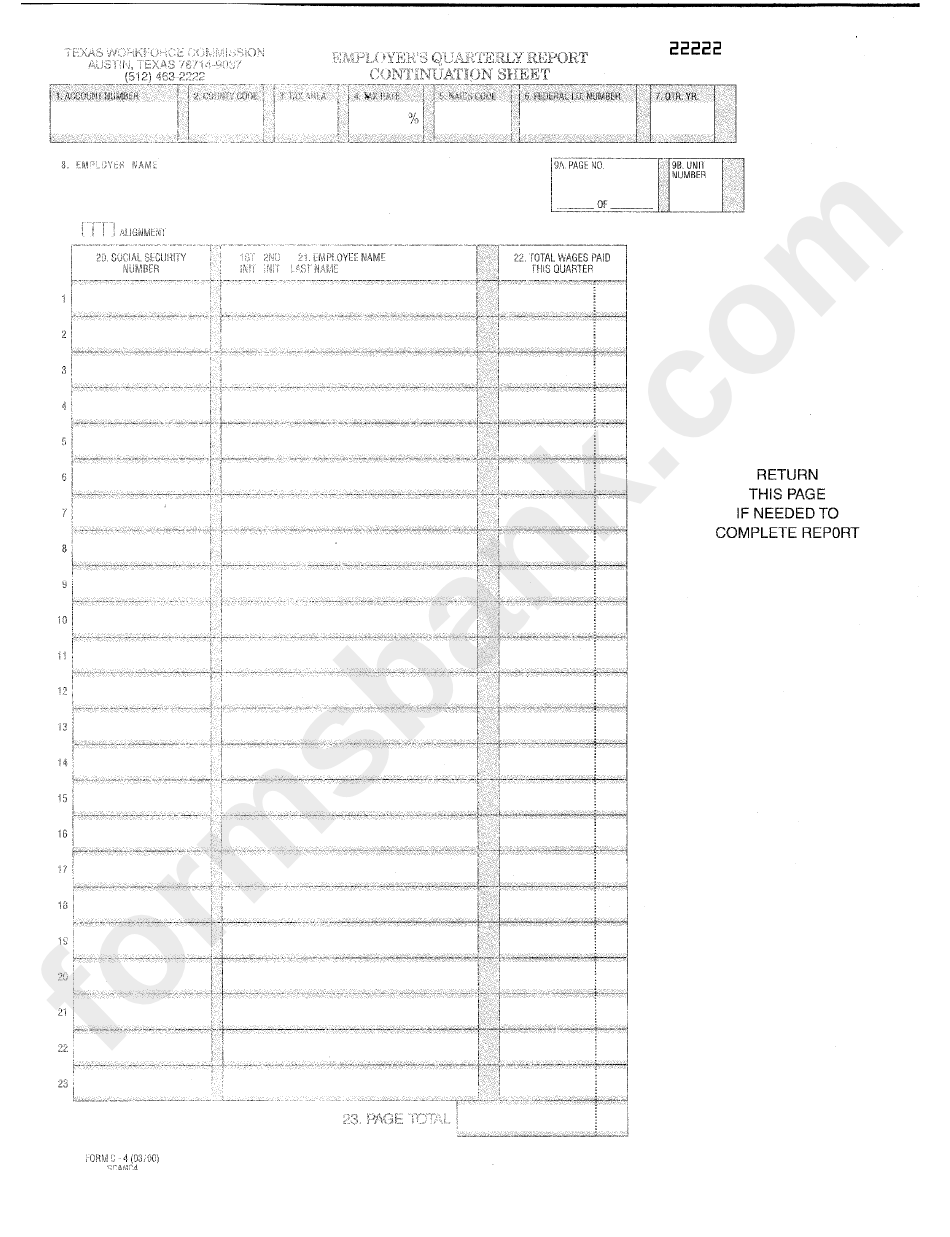
Form C4 Employer'S Quarterly Report Continuation Sheet printable pdf
(to report the first time you treated the patient,. The physician fills out their part of the form, and sends a copy to your employer and the. Address insurer's use only city state zip provider's tax i.d. Web 1.this form is used for a workers' compensation, volunteer firefighters' or volunteer ambulance workers' benefit case as follows: Web attach to form.
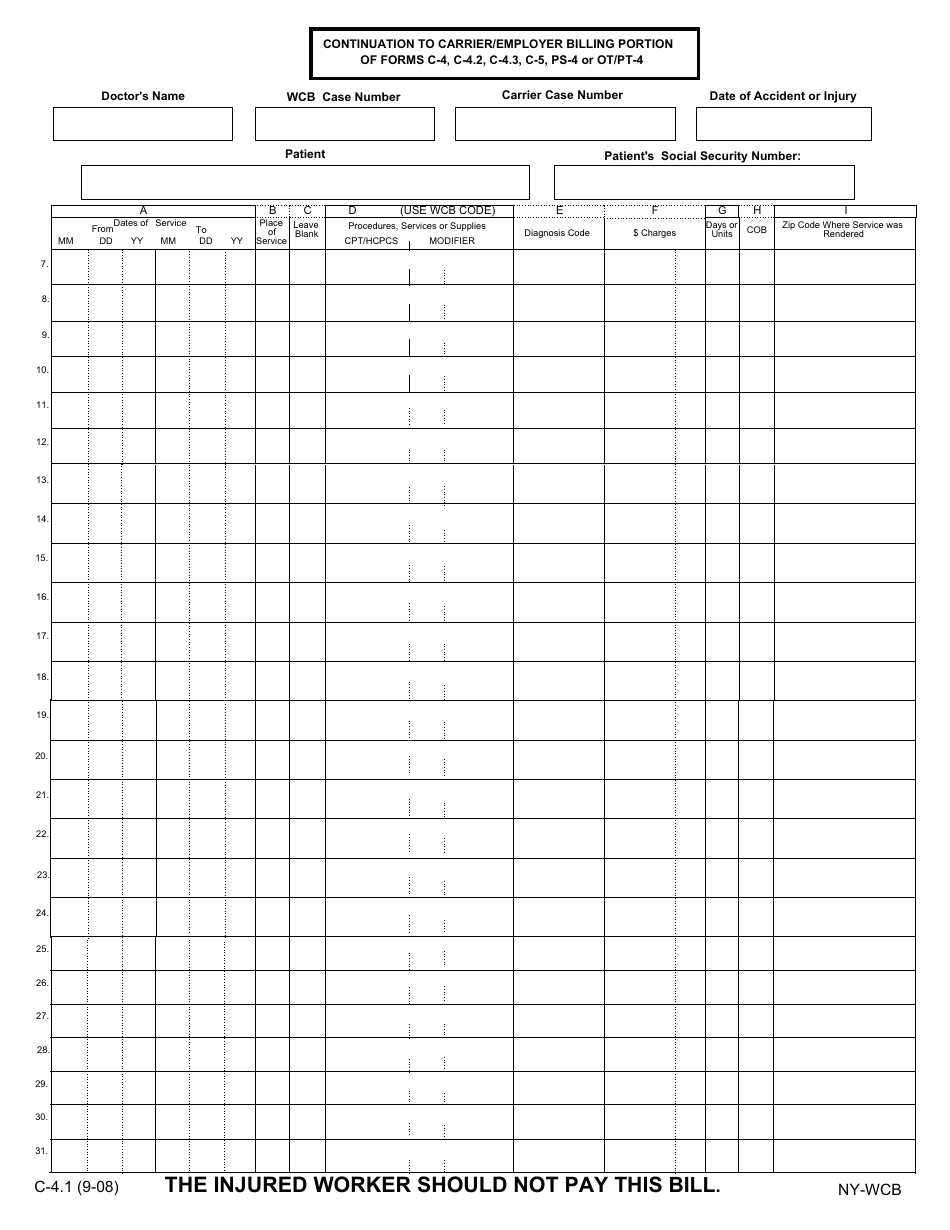
Form C4.1 Download Fillable PDF or Fill Online Continuation to Carrier
Make sure that you review his entries before you leave the hospital. See instructions for schedule c (form 1040). Workers compensation c 4 form is a form that you must fill out to get workers compensation. (to report the first time you treated the patient,. Form 4720, return of certain excise taxes on charities and other persons.
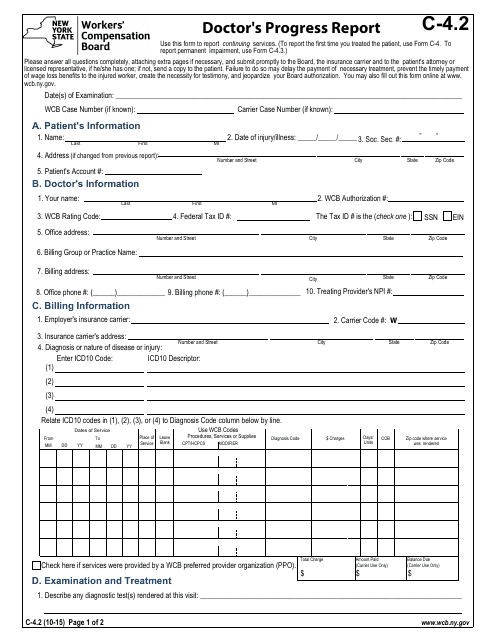
Form C4.2 Download Fillable PDF or Fill Online Doctor's Progress
(to report the first time you treated the patient,. Web form full name social security number (last) (first) (mi) home address (number and street) (city) (state) (zip code) as an employee of auburn university, my total compensation is. Workers compensation c 4 form is a form that you must fill out to get workers compensation. When completing section 2, use.

100x DIN 7982 SenkkopfBlechschraube Form C 4.8 x 25 Stahl galv
[noun] a high explosive composed of various chemicals that make it moldable and plastic. Web 1.this form is used for a workers' compensation, volunteer firefighters' or volunteer ambulance workers' benefit case as follows: (to report the first time you treated the patient,. When completing section 2, use information from the documentation the. Employer or authorized representative review and verification.
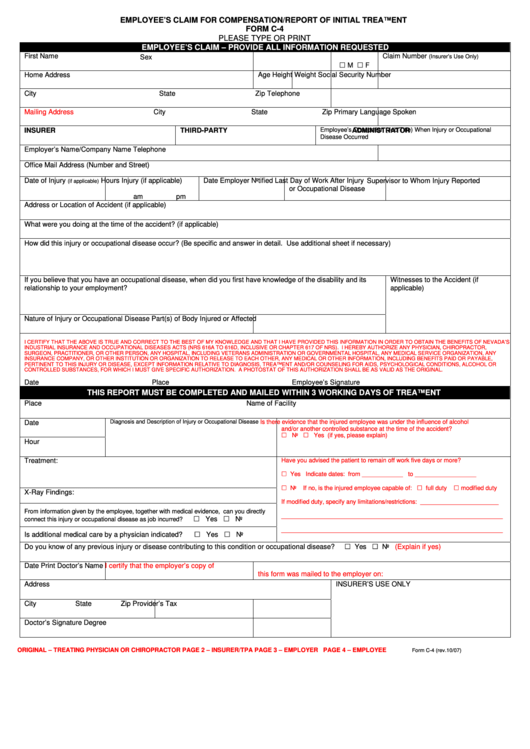
Form C4 Employee'S Claim For Compensation/report Of Initial
Web use this form when a patient has reached maximum medical improvement and to render an opinion on permanent impairment, if any. The physician fills out their part of the form, and sends a copy to your employer and the. [noun] a high explosive composed of various chemicals that make it moldable and plastic. 09 name of proprietor social security.
Employer Or Authorized Representative Review And Verification.
Address insurer's use only city state zip provider's tax i.d. The physician fills out their part of the form, and sends a copy to your employer and the. [noun] a high explosive composed of various chemicals that make it moldable and plastic. To confirm a telephone request for written.
This Committee Has Qualified As A Multicandidate Committee (See Fec Form 1M) 4.
Web date, sign, and list the facility you went to. To start the form, utilize the fill camp; Make sure that you review his entries before you leave the hospital. Form 4720, return of certain excise taxes on charities and other persons.
This Form Must Be Attached To And Filed.
This appendix contains ten sample notification forms. Web use this form to report continuing services. Fill, sign, print and send online instantly. See instructions for schedule c (form 1040).
Web 1 Day Agofec Committee Id #:
Web use this form when a patient has reached maximum medical improvement and to render an opinion on permanent impairment, if any. Web form full name social security number (last) (first) (mi) home address (number and street) (city) (state) (zip code) as an employee of auburn university, my total compensation is. When completing section 2, use information from the documentation the. Sign online button or tick the preview image of the document.