Injectafer Order Form
Injectafer Order Form - Web injectafer treatment may be repeated if ida or iron deficiency in heart failure reoccurs. Diagnosis and icd 10 code iron deficiency anemia icd 10 code: Web provider order form rev. If extravasation occurs, discontinue the injectafer administration at that site. Check request form all documentation can also be mailed to: Injectafer treatment may be repeated if ida reoccurs. Web injectafer® (ferric carboxymaltose) order form please include the following (required): If you have questions about injectafer support, call: Initial appointment date and time will be verified after insurance approval. Check request form this form is used by the office in the event there is an issue with the processing of the injectafer ® savings program financial card.
750 mg (>50 kg) or 15 mg/kg (<50kg) frequency: Check request form all documentation can also be mailed to: Web provider order form rev. Web please fax with this order form. Web injectafer treatment may be repeated if ida or iron deficiency in heart failure reoccurs. Web how do i make a referral or transition my treatment to infusion associates? (2.3) _____ dosage forms and strengths_____ injection: Web referralform you have selected injectafer for your patient, please fill out this form and fax it to the infusing practice or center. Providers can find order forms on our medications page. Be sure to attach a copy of your patient’s insurance information and currentdear healthcarelab values.provider:
Injectafer treatment may be repeated if ida reoccurs. Give 2 doses separated by at least 7 days, each iv dose of 750mg in 250mls. Web this form is used by the office in the event there is an issue with the processing of the injectafer ® savings program financial card. Web injectafer treatment may be repeated if ida or iron deficiency in heart failure reoccurs. Web how do i make a referral or transition my treatment to infusion associates? Cbc within the last 6 months (if outside of atrium, please fax with order, required prior to scheduling) infusion therapy: Be sure to attach a copy of your patient’s insurance information and currentdear healthcarelab values.provider: Web for patients weighing lessthan 50kg (110lb): Initial appointment date and time will be verified after insurance approval. *list of infusion center locations may be found at:

Injectafer side effects What they are and how to manage them
*list of infusion center locations may be found at: Utah providers fax form to: Check request form this form is used by the office in the event there is an issue with the processing of the injectafer ® savings program financial card. Injectafer treatment may be repeated if ida reoccurs. Once weekly x 2 weeks total cumulative dose up to.

Injectafer Lawsuits Compensation For Hypophosphatemia Side Effects
New to therapy continuing therapy last treatment date: Web injectafer® (ferric carboxymaltose) order form please include the following (required): Please fax completed order, along with referral form to desired location. Patient demographics & insurance information 2. Web avoid extravasation of injectafer since brown discoloration of the extrav asation site may be long lasting.

Sales Order Templates Excel 2 Latest Tips You Can Learn When Attending
Injectafertreatment may be repeated if iron deficiency anemia r eoccurs. New to therapy continuing therapy last treatment date: Providers can find order forms on our medications page. Patient demographics & insurance information. Please include the following (required):

Injectafer Lawsuit Free Evaluation James Scott Farrin
Web avoid extravasation of injectafer since brown discoloration of the extrav asation site may be long lasting. Web for patients weighing lessthan 50kg (110lb): New referral updated order order renewal date: Utah providers fax form to: Discover the benefits of injectafer more iron in less time *
Injectafer Dangerous Side Effects Investigation Migliaccio & Rathod LLP
Diagnosis and icd 10 code iron deficiency anemia icd 10 code: Please include the following (required): Patient demographics & insurance information 2. Download in english download in spanish. *list of infusion center locations may be found at:
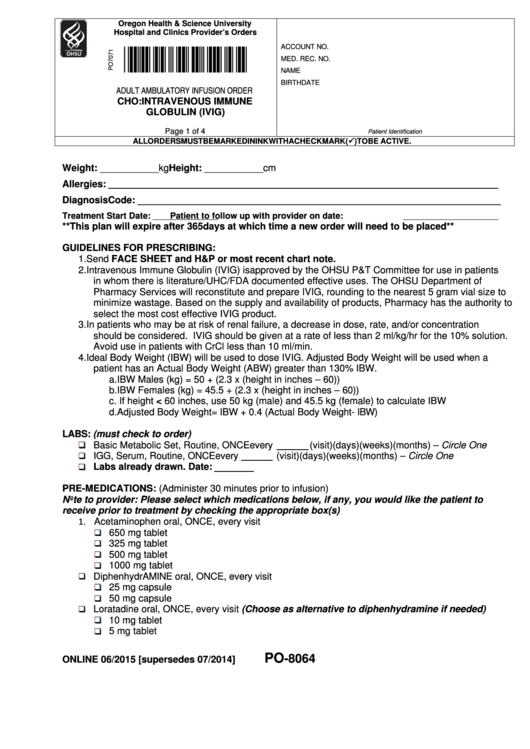
Adult Ambulatory Infusion Order Form Cho Intravenous Immune Globulin
An iron infusion is a procedure in which iron is delivered to your body intravenously, meaning into a vein through a. Web injectafer is an intravenous (iv) iron replacement product used to treat ida. New to therapy continuing therapy last treatment date: 750 mg (>50 kg) or 15 mg/kg (<50kg) frequency: Be sure to attach a copy of your patient’s.
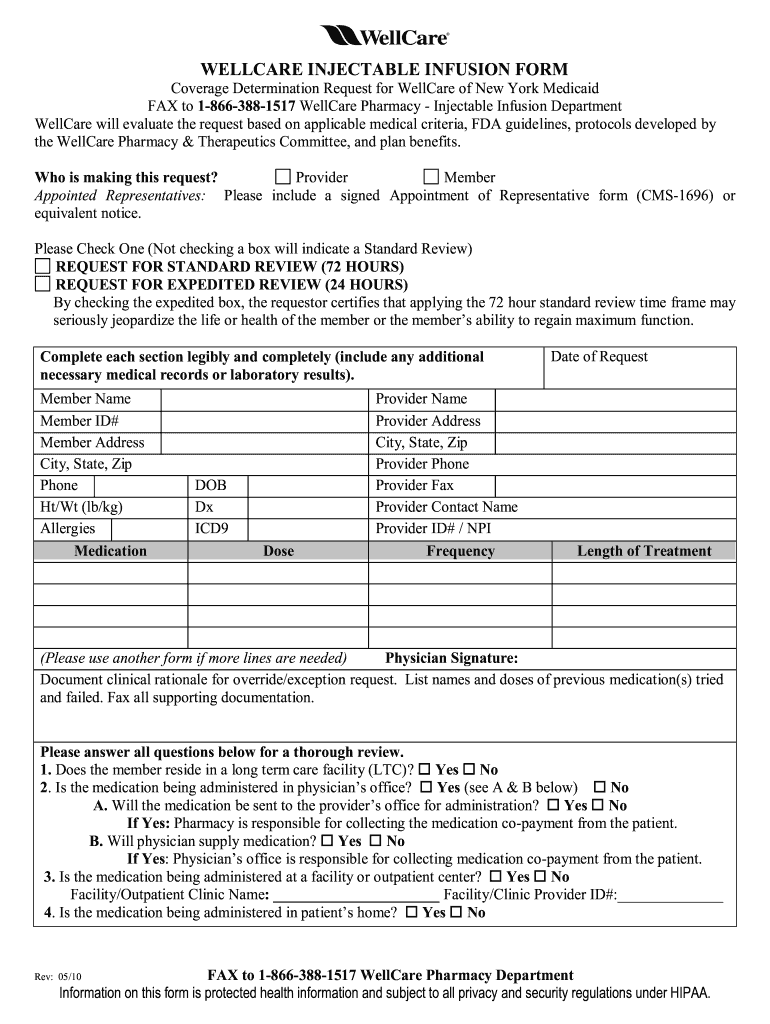
WellCare Injectable Infusion Form 20102022 Fill and Sign Printable
Download in english download in spanish. 750 mg (>50 kg) or 15 mg/kg (<50kg) frequency: Injectafer treatment may be repeated if ida reoccurs. Web injectafer (ferric carboxymaltose) iv dosing dose: Utah providers fax form to:

Injectafer Class Action Lawsuit Injectafer Infusion Lawyer
If extravasation occurs, discontinue the injectafer administration at that site. Web how do i make a referral or transition my treatment to infusion associates? Please fax completed order, along with referral form to desired location. Be sure to attach a copy of your patient’s insurance information and currentdear healthcarelab values.provider: Requests will be accommodated based on infusion center availability and.

PPINUS0139 2018 Fill and Sign Printable Template Online US Legal
Injectafer treatment may be repeated if ida reoccurs. An iron infusion is a procedure in which iron is delivered to your body intravenously, meaning into a vein through a. Check request form all documentation can also be mailed to: 1/6/2023 patient information referral status: Diluted in sodium chloride 0.9 % iv as directed over at least 30 minutes weight less.

Injectafer Uses, How It Works, Precautions and Warnings
*list of infusion center locations may be found at: Utah providers fax form to: Injectafertreatment may be repeated if iron deficiency anemia r eoccurs. It was designed to slowly release iron once inside your body, which may decrease the potential for some side effects and give you more iron in just 2 administrations. (1 dx has to be iron deficiency.
Initial Appointment Date And Time Will Be Verified After Insurance Approval.
*list of infusion center locations may be found at: New to therapy continuing therapy last treatment date: Web please fax with this order form. Web avoid extravasation of injectafer since brown discoloration of the extrav asation site may be long lasting.
If Extravasation Occurs, Discontinue The Injectafer Administration At That Site.
Providers can find order forms on our medications page. It was designed to slowly release iron once inside your body, which may decrease the potential for some side effects and give you more iron in just 2 administrations. Select a program to see how it could help your patients. Check request form all documentation can also be mailed to:
Download In English Download In Spanish.
An iron infusion is a procedure in which iron is delivered to your body intravenously, meaning into a vein through a. Injectafer treatment may be repeated if ida reoccurs. Requests will be accommodated based on infusion center availability and are not guaranteed. Please fax completed order, along with referral form to desired location.
Once Weekly X 2 Weeks Total Cumulative Dose Up To 1500 Mg Per Course Qualifiers **2 Diagnoses Needed For Insurance Approval And Coverage.
Patient demographics & insurance information. Utah providers fax form to: New referral updated order order renewal date: (1 dx has to be iron deficiency anemia, 2 dx the cause of anemia)