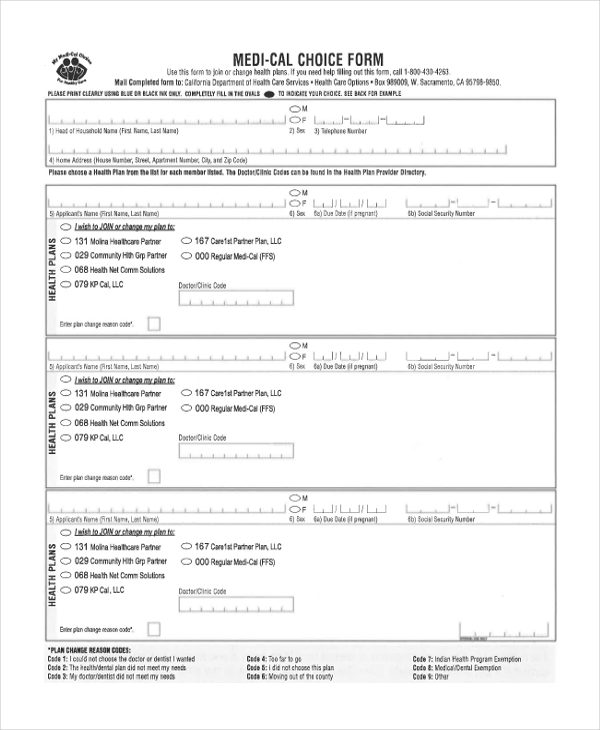
Medi Cal Choice Form Pdf
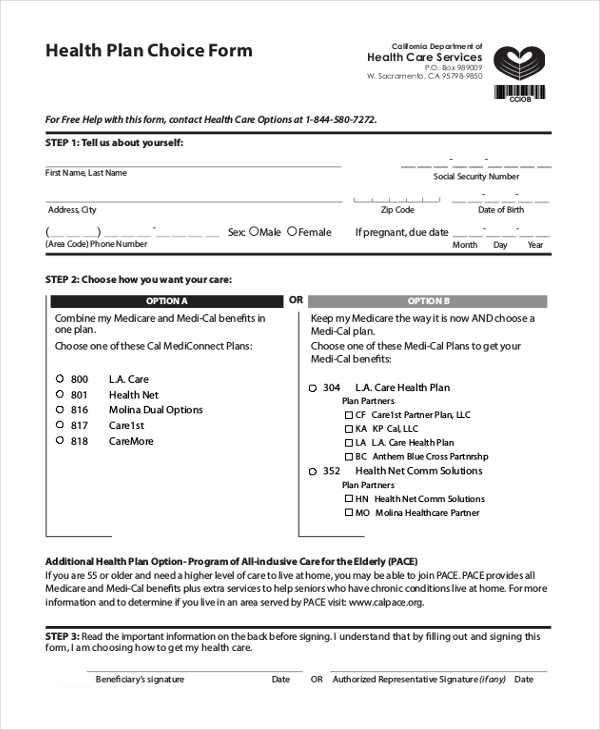
Medi Cal Choice Form Pdf - If you need a printed version of a document, a printed. Health insurance premium program (hipp) application. Easily fill out pdf blank, edit, and sign them. Use this complete the top part of the form (name, the next part of the form is about each person in fill in the oval next to california. Web request a print or alternate format document. Web for a list of mced forms by form number, please click on the following link: Scfhp documents are available below for easy viewing and download. Web the way to fill out the filling out medicalchoice form on the internet: Web health plan choice form if you do not want to automatically enroll in the cal mediconnect plan we have chosen for you, use this form to choose a different option. You can get more forms by calling.
Save or instantly send your ready documents. Sign online button or tick the preview image of the document. For information about completing and submitting these forms, please review the appropriate provider. Easily fill out pdf blank, edit, and sign them. If you need a printed version of a document, a printed. To get started on the form, use the fill camp; You need help filling out. Web the way to fill out the filling out medicalchoice form on the internet: Enter your search criteria in the fields. California department of health care services p.o.
Web the way to fill out the filling out medicalchoice form on the internet: Fill out one form for each family member. Web health plan choice form if you do not want to automatically enroll in the cal mediconnect plan we have chosen for you, use this form to choose a different option. For a list of translated mced forms by language, please click on the following link:. Sign online button or tick the preview image of the document. Web request a print or alternate format document. You can get more forms by calling. You need help filling out. Health insurance premium payment program. Save or instantly send your ready documents.

MediCal小冊子 『My MediCal Choice For Healthy Care』大解説 ドクターの選択とフォームの記入
Scfhp documents are available below for easy viewing and download. You can get more forms by calling. Health insurance premium payment program. For information about completing and submitting these forms, please review the appropriate provider. You need help filling out.
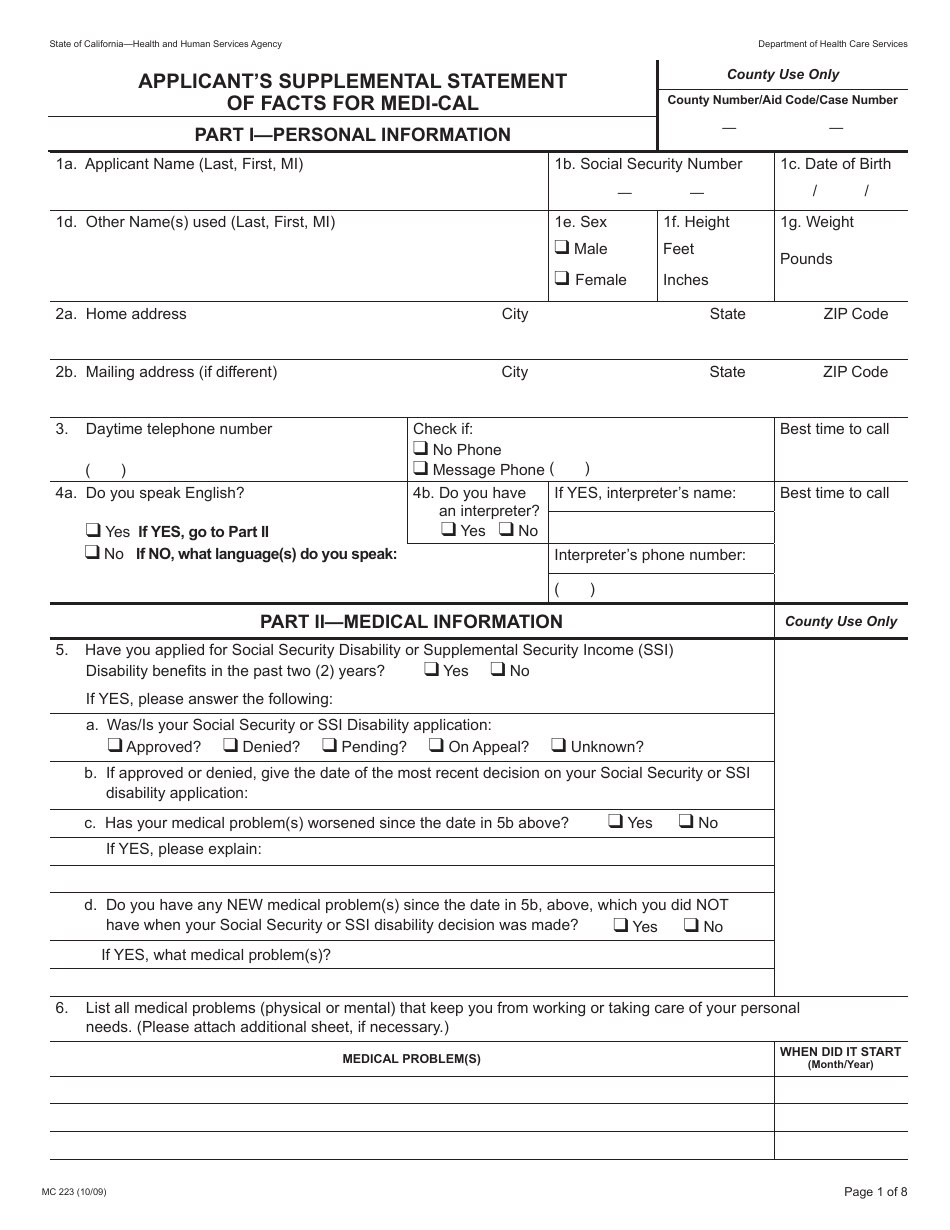
Form MC223 Download Printable PDF or Fill Online Applicant's
Web health plan choice form if you do not want to automatically enroll in the cal mediconnect plan we have chosen for you, use this form to choose a different option. For information about completing and submitting these forms, please review the appropriate provider. For a list of translated mced forms by language, please click on the following link:. If.
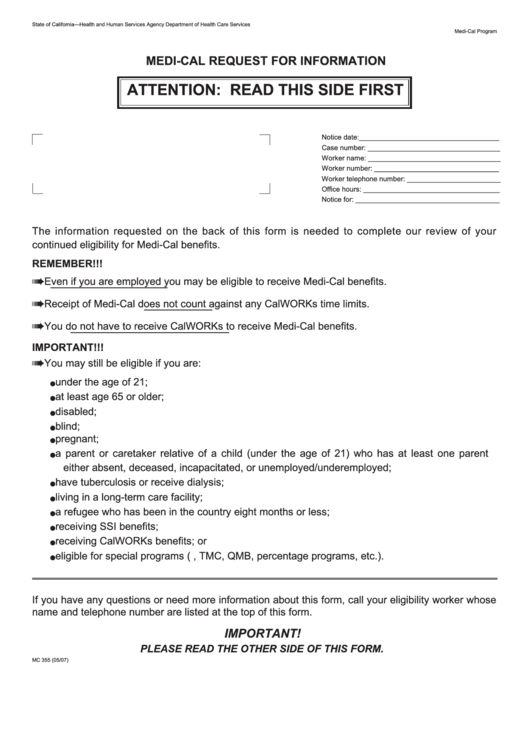
Fillable MediCal Request For Information printable pdf download
Health insurance premium payment program. Save or instantly send your ready documents. If you need a printed version of a document, a printed. Scfhp documents are available below for easy viewing and download. View and download frequently used forms, brochures, guides, and other information related to products and eligibility.
Medi Cal Choice Form Doctor Clinic Code
California department of health care services p.o. Web health plan choice form if you do not want to automatically enroll in the cal mediconnect plan we have chosen for you, use this form to choose a different option. If you need a printed version of a document, a printed. Enter your search criteria in the fields. Save or instantly send.
FREE 9+ Sample Medical Choice Forms in PDF MS Word
Use this complete the top part of the form (name, the next part of the form is about each person in fill in the oval next to california. Web mail form back to: Enter your search criteria in the fields. Web health plan choice form if you do not want to automatically enroll in the cal mediconnect plan we have.
Medical Choice Form ≡ Fill Out Printable PDF Forms Online
Web health plan choice form if you do not want to automatically enroll in the cal mediconnect plan we have chosen for you, use this form to choose a different option. Health insurance premium program (hipp) application. For a list of translated mced forms by language, please click on the following link:. Web for a list of mced forms by.
Fillable Form Mc 212 MediCal Residency Declaration (Declaracion De
For a list of translated mced forms by language, please click on the following link:. Easily fill out pdf blank, edit, and sign them. If you need a printed version of a document, a printed. Web request a print or alternate format document. Health insurance premium program (hipp) application.
2014 Form AU NAT 13080 Fill Online, Printable, Fillable, Blank pdfFiller
Save or instantly send your ready documents. Sign online button or tick the preview image of the document. Use this complete the top part of the form (name, the next part of the form is about each person in fill in the oval next to california. Enter your search criteria in the fields. You can get more forms by calling.

Fill Free fillable MEDICAL CHOICE FORM 300 Alameda Alliance for
Scfhp documents are available below for easy viewing and download. To get started on the form, use the fill camp; Easily fill out pdf blank, edit, and sign them. Web for a list of mced forms by form number, please click on the following link: For a list of translated mced forms by language, please click on the following link:.

Addressing the New MediCal Expansion & Immigrant Health Town Hall
Scfhp documents are available below for easy viewing and download. Sign online button or tick the preview image of the document. Easily fill out pdf blank, edit, and sign them. You can get more forms by calling. Enter your search criteria in the fields.
Use This Complete The Top Part Of The Form (Name, The Next Part Of The Form Is About Each Person In Fill In The Oval Next To California.
Save or instantly send your ready documents. Web for a list of mced forms by form number, please click on the following link: If you need a printed version of a document, a printed. You need help filling out.
You Will Also Learn What.
California department of health care services p.o. Health insurance premium program (hipp) application. Scfhp documents are available below for easy viewing and download. Web estate recovery forms.
You Can Get More Forms By Calling.
Web health plan choice form if you do not want to automatically enroll in the cal mediconnect plan we have chosen for you, use this form to choose a different option. To get started on the form, use the fill camp; Fill out one form for each family member. Health insurance premium payment program.
Web Mail Form Back To:
For information about completing and submitting these forms, please review the appropriate provider. View and download frequently used forms, brochures, guides, and other information related to products and eligibility. For a list of translated mced forms by language, please click on the following link:. Enter your search criteria in the fields.