Nevada C4 Form
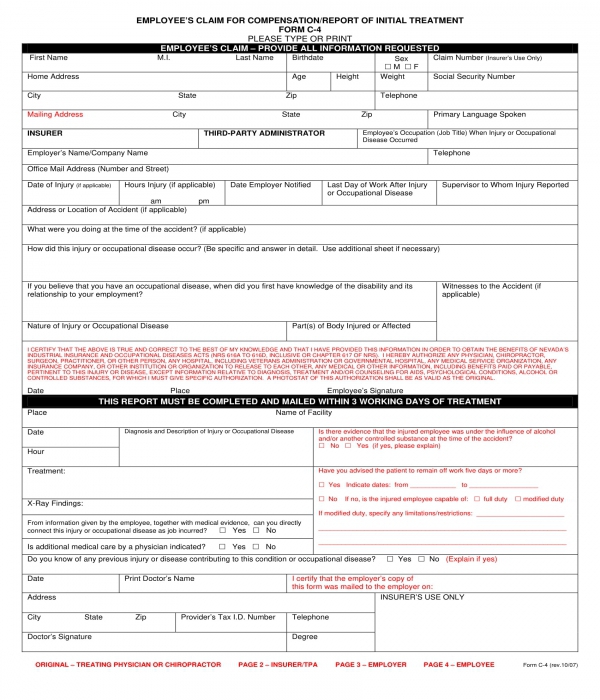
Nevada C4 Form - If different from mailing address telephone city state zip insurer third. For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free: How can my office staff locate the correct insurer/tpa? You must send the completed form. Employer’s report of industrial injury or occupational disease employer employer’s name nature of business (mfg., etc.) fein osha log # office mail address location. Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number
How can my office staff locate the correct insurer/tpa? If different from mailing address telephone city state zip insurer third. Employer’s report of industrial injury or occupational disease employer employer’s name nature of business (mfg., etc.) fein osha log # office mail address location. Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number You must send the completed form. Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free:
Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free: How can my office staff locate the correct insurer/tpa? You must send the completed form. Employer’s report of industrial injury or occupational disease employer employer’s name nature of business (mfg., etc.) fein osha log # office mail address location. If different from mailing address telephone city state zip insurer third. Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number

Form C4 2 ≡ Fill Out Printable PDF Forms Online
If different from mailing address telephone city state zip insurer third. Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number How can my office staff locate the correct insurer/tpa? You must.
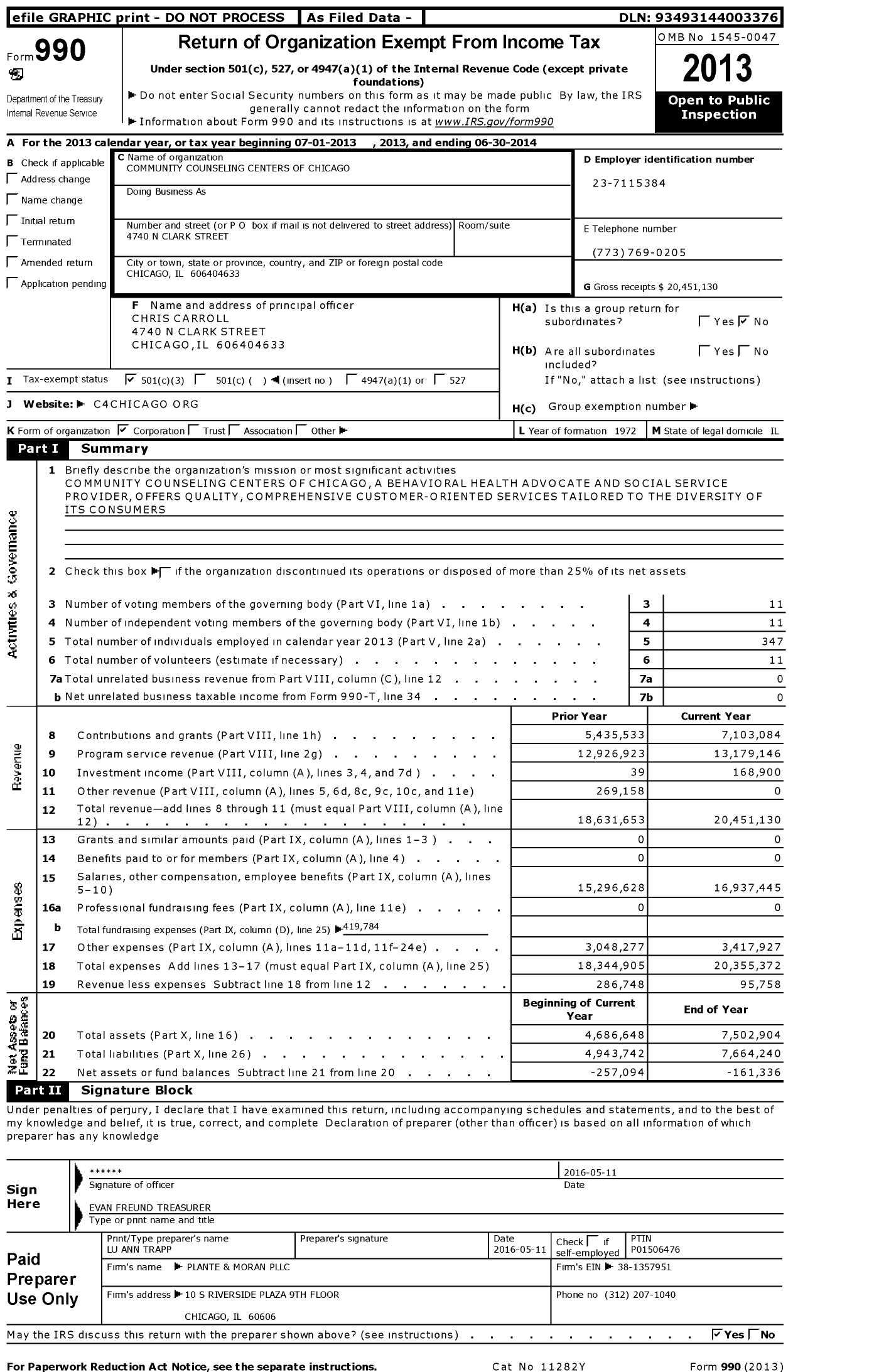
2014 Form 990 for Community Counseling Centers of Chicago (C4) Cause IQ
You must send the completed form. Employer’s report of industrial injury or occupational disease employer employer’s name nature of business (mfg., etc.) fein osha log # office mail address location. Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number How can my office staff locate the correct insurer/tpa? Last name.

C4+C5 Set for flowform rivets RAE Reliable Automotive Equipment, Inc.
Employer’s report of industrial injury or occupational disease employer employer’s name nature of business (mfg., etc.) fein osha log # office mail address location. If different from mailing address telephone city state zip insurer third. Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number How can my office staff locate.

Nevada Mountains 120306141850 C4 Snow covered Nevada Moun… Flickr
If different from mailing address telephone city state zip insurer third. Employer’s report of industrial injury or occupational disease employer employer’s name nature of business (mfg., etc.) fein osha log # office mail address location. For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free: You must send the completed.
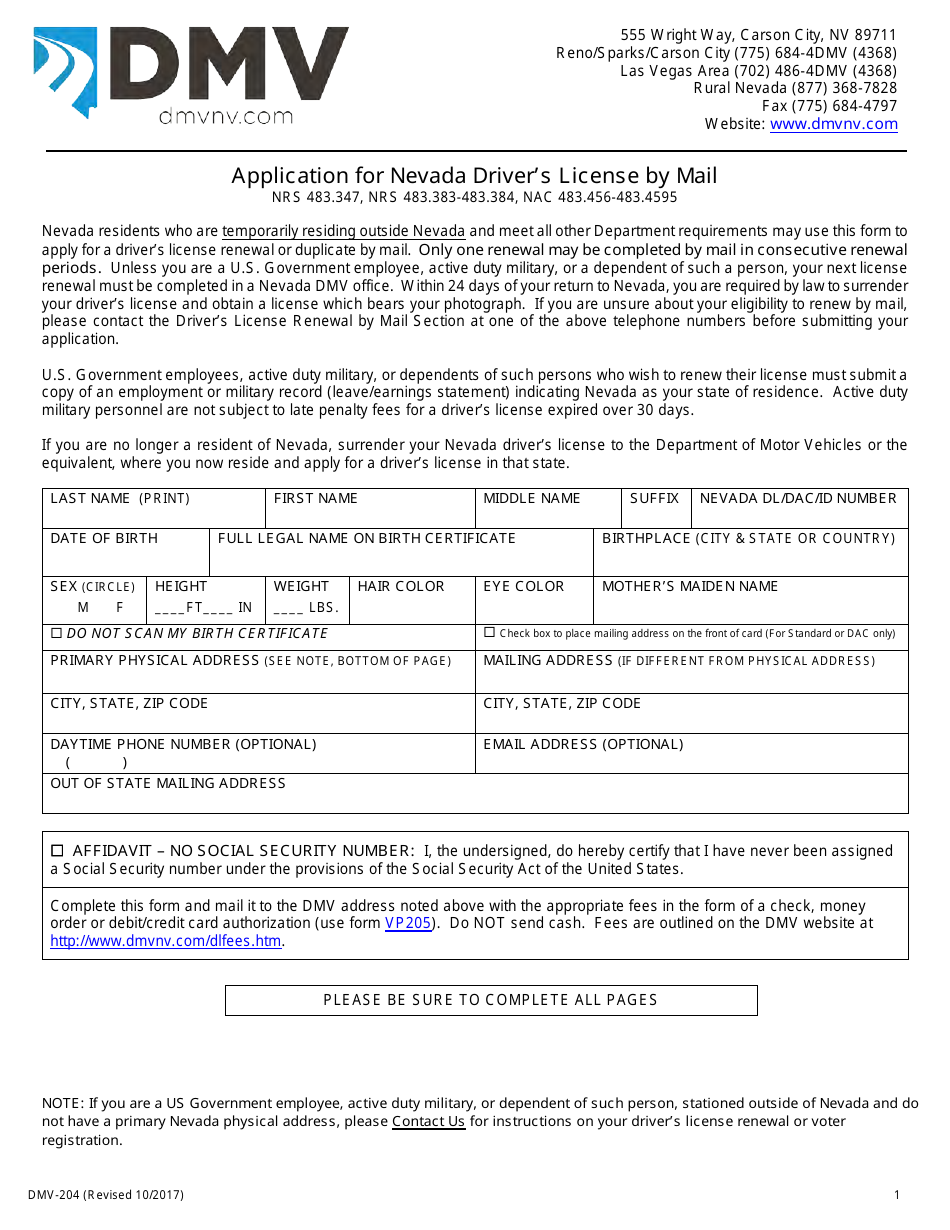
Form DMV204 Download Fillable PDF or Fill Online Application for
For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free: How can my office staff locate the correct insurer/tpa? Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number If different from mailing address telephone city state zip insurer third. Last.

c4 MINPINERIE
Employer’s report of industrial injury or occupational disease employer employer’s name nature of business (mfg., etc.) fein osha log # office mail address location. If different from mailing address telephone city state zip insurer third. For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free: Last name birthdate sex m.
FREE 7+ Compensation and Benefits Forms in PDF
For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free: If different from mailing address telephone city state zip insurer third. Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number Last name birthdate sex m f claim number (insurer’s use.
State Of Nevada Combined Sales And Use Tax Return Form Form Resume
Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free: Employer’s report of industrial injury or occupational disease employer employer’s name nature of business (mfg., etc.) fein osha log # office.

20152020 Form NY C4.3 Fill Online, Printable, Fillable, Blank pdfFiller
Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number If different from mailing address telephone city state zip insurer third. For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free: Employer’s report of industrial injury or occupational disease employer employer’s.
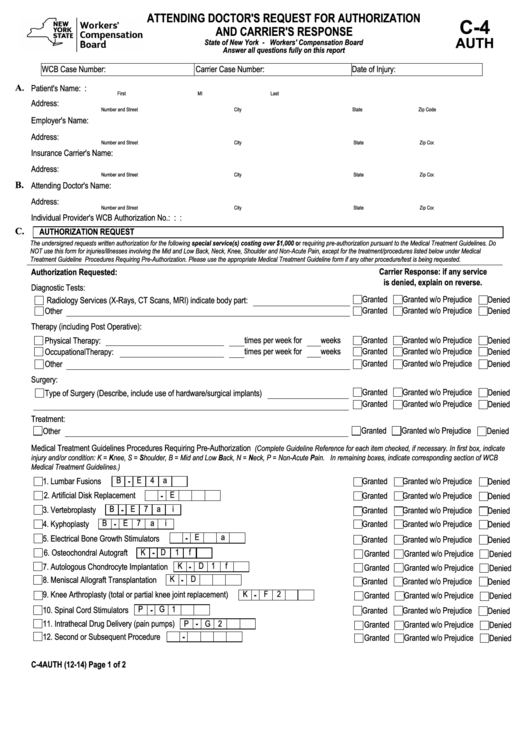
Fillable C4 Auth Workers' Compensation Board printable pdf download
If different from mailing address telephone city state zip insurer third. Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number How can my office staff locate the correct insurer/tpa? For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free: Last.
Last Name Birthdate Sex M F Claim Number (Insurer’s Use Only) Home Address Age Height Weight Social Security Number
You must send the completed form. Last name birthdate sex m f claim number (insurer’s use only) home address age height weight social security number For assistance with workers’ compensation issues you may contact the state of nevada office for consumer health assistance toll free: If different from mailing address telephone city state zip insurer third.
How Can My Office Staff Locate The Correct Insurer/Tpa?
Employer’s report of industrial injury or occupational disease employer employer’s name nature of business (mfg., etc.) fein osha log # office mail address location.