Novo Nordisk Pap Refill Form
Novo Nordisk Pap Refill Form - The patient assistance program provides medication at no cost to those who qualify. All information must be completed unless otherwise indicated. Web novo nordisk patient assistance program refill/reorder request form must be submitted directly by the hcp and must include a cover letter/hcp letterhead to clearly identify hcp as the sender. Reserves the right to modify or cancel this program at any time without notice. Web the novo nordisk patient assistance program (pap) is based on our commitment to our patients. (iv) investigating and verifying my insurance benefits; Web renewal the novo nordisk hormone therapy patient assistance program (pap) provides medication to eligible applicants at no charge. (v) coordinating the dispensing and delivery of medication; Patients who are approved for the pap may qualify to. (iii) identifying and/or determining eligibility under pap and other patient assistance resources;
Web renewal the novo nordisk hormone therapy patient assistance program (pap) provides medication to eligible applicants at no charge. Novo nordisk patient assistance program hormone therapy po box 181640 louisville, ky 40261 novo nordisk inc. (v) coordinating the dispensing and delivery of medication; Web the novo nordisk patient assistance program (pap) is based on our commitment to our patients. Web this personal information aids in administering pap by: Patients can renew each year for as long as they qualify. Reserves the right to modify or cancel this program at any time without notice. All information must be completed unless otherwise indicated. Web novo nordisk patient assistance program application instructions for completing the application complete all fields to avoid return of incomplete application make sure the application is signed by the prescriber and dated remember to include disposable pen needles in the order information if applicable For uninsured patients, an approved application is valid for 12 months.
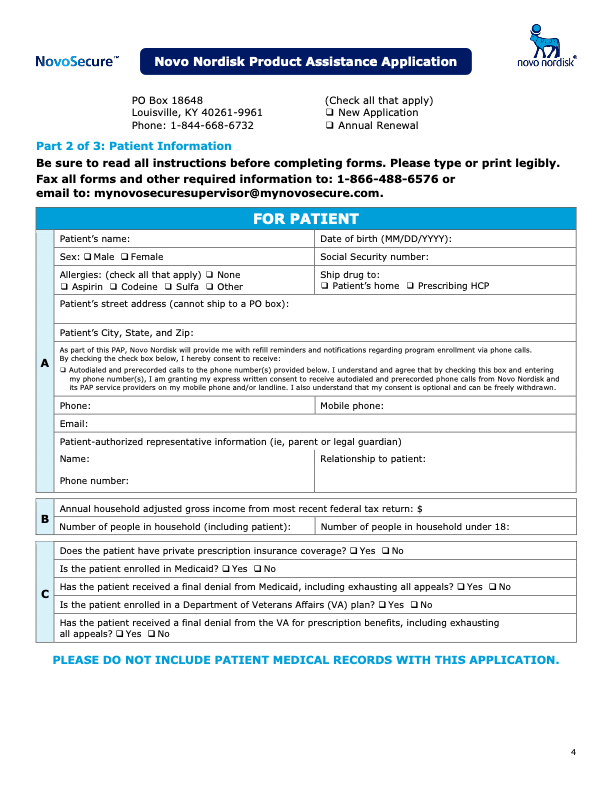
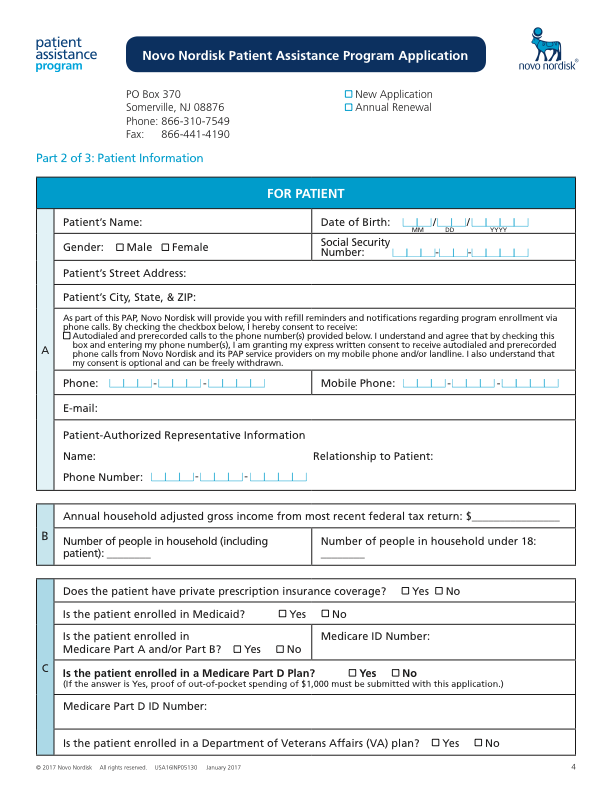
Web this personal information aids in administering pap by: Novo nordisk patient assistance program hormone therapy po box 181640 louisville, ky 40261 novo nordisk inc. Reserves the right to modify or cancel this program at any time without notice. Web novo nordisk patient assistance program application instructions for completing the application complete all fields to avoid return of incomplete application make sure the application is signed by the prescriber and dated remember to include disposable pen needles in the order information if applicable (iv) investigating and verifying my insurance benefits; After you have finished entering information, this form will be sent to your patient or their caregiver who will need to fill out their sections of the form as well. Web novo nordisk patient assistance program refill/reorder request form must be submitted directly by the hcp and must include a cover letter/hcp letterhead to clearly identify hcp as the sender. Web novo nordisk patient assistance program (pap) available products victoza® (liraglutide) injection 1.2 mg 2 pen pack* victoza® (liraglutide) injection 1.8 mg 3 pen pack* ozempic® (semaglutide) injection pen that delivers doses of 0.25 mg or 0.5 mg Patients who are approved for the pap may qualify to. (iii) identifying and/or determining eligibility under pap and other patient assistance resources;
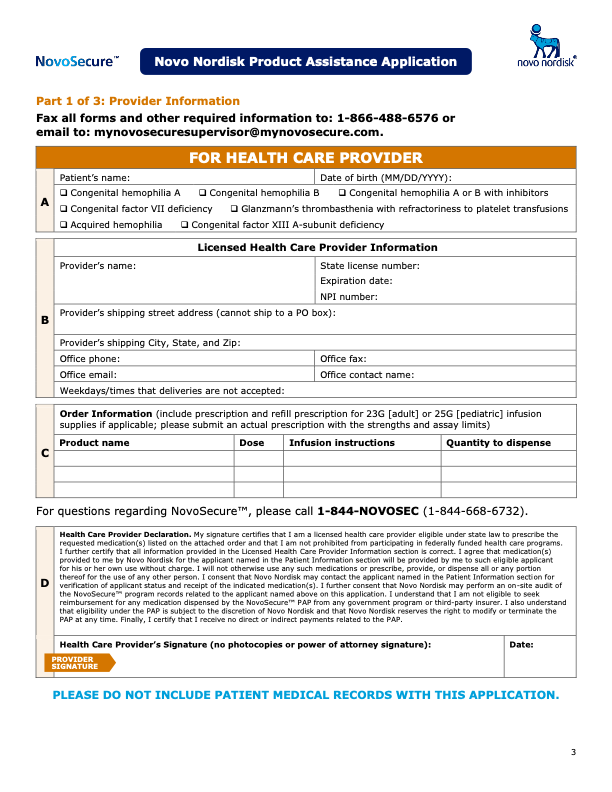
Product Assistance Program Novoeight® (Antihemophilic Factor
Web this personal information aids in administering pap by: Reserves the right to modify or cancel this program at any time without notice. The patient assistance program provides medication at no cost to those who qualify. Novo nordisk patient assistance program hormone therapy po box 181640 louisville, ky 40261 novo nordisk inc. (v) coordinating the dispensing and delivery of medication;
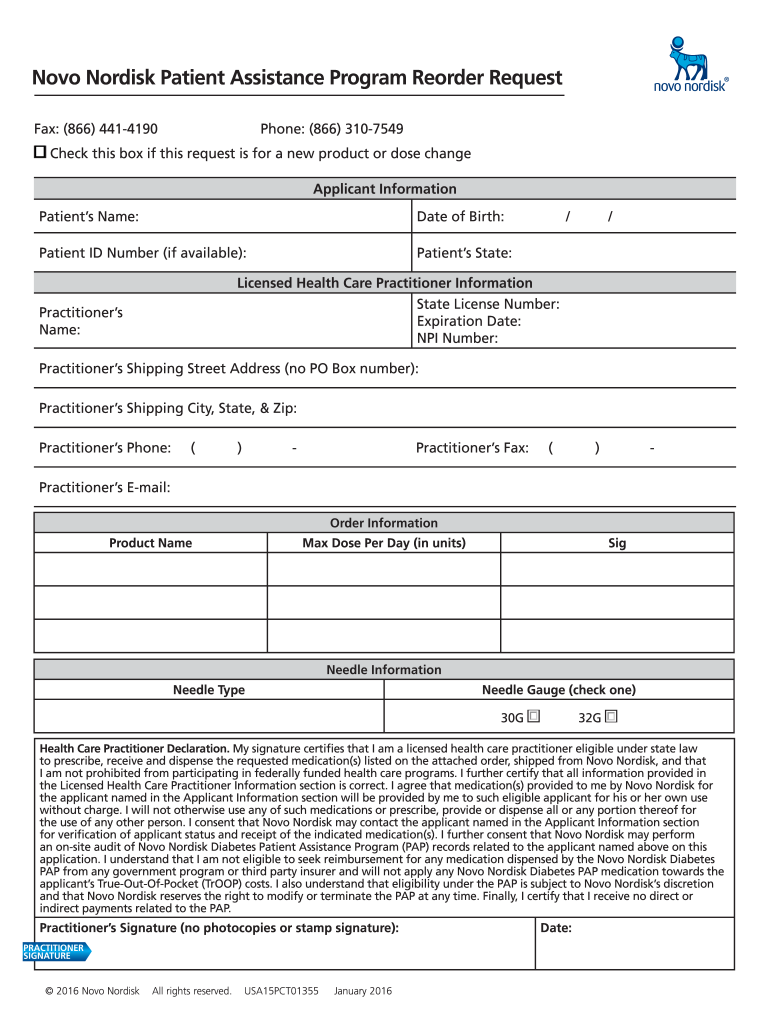
Novo Nordisk Refill Form 2021 Fill Online, Printable, Fillable, Blank
Patients who are approved for the pap may qualify to. (iii) identifying and/or determining eligibility under pap and other patient assistance resources; For uninsured patients, an approved application is valid for 12 months. Web renewal the novo nordisk hormone therapy patient assistance program (pap) provides medication to eligible applicants at no charge. Web novo nordisk patient assistance program (pap) available.

Novo Nordisk to boost pillform diabetic drugs with 1.8 billion deal
After you have finished entering information, this form will be sent to your patient or their caregiver who will need to fill out their sections of the form as well. Web novo nordisk patient assistance program application instructions for completing the application complete all fields to avoid return of incomplete application make sure the application is signed by the prescriber.
Novo Nordisk PAP How To Get A Free 90 Day Supply of Insulin (2021)
(v) coordinating the dispensing and delivery of medication; Patients who are approved for the pap may qualify to. Patients can renew each year for as long as they qualify. Reserves the right to modify or cancel this program at any time without notice. Web renewal the novo nordisk hormone therapy patient assistance program (pap) provides medication to eligible applicants at.
Product Assistance Program Novoeight® (Antihemophilic Factor
Web this personal information aids in administering pap by: Novo nordisk patient assistance program hormone therapy po box 181640 louisville, ky 40261 novo nordisk inc. All information must be completed unless otherwise indicated. The patient assistance program provides medication at no cost to those who qualify. Web novo nordisk patient assistance program (pap) available products victoza® (liraglutide) injection 1.2 mg.
NovoNordisk_logo SoftconsuLt
Novo nordisk patient assistance program hormone therapy po box 181640 louisville, ky 40261 novo nordisk inc. Web the novo nordisk patient assistance program (pap) is based on our commitment to our patients. Web novo nordisk patient assistance program application instructions for completing the application complete all fields to avoid return of incomplete application make sure the application is signed by.
Product Assistance Program Novoeight® (Antihemophilic Factor
Web novo nordisk patient assistance program application instructions for completing the application complete all fields to avoid return of incomplete application make sure the application is signed by the prescriber and dated remember to include disposable pen needles in the order information if applicable Novo nordisk patient assistance program hormone therapy po box 181640 louisville, ky 40261 novo nordisk inc..

Insulin Aspart Pen at Rs 2800/pack इंसुलिन पेन Aggarwal Pharma, New
Patients who are approved for the pap may qualify to. Web this personal information aids in administering pap by: Web novo nordisk patient assistance program (pap) available products victoza® (liraglutide) injection 1.2 mg 2 pen pack* victoza® (liraglutide) injection 1.8 mg 3 pen pack* ozempic® (semaglutide) injection pen that delivers doses of 0.25 mg or 0.5 mg The patient assistance.

Buy Norditropin 45 IU Somatropin (rDNA origin) Novo Nordisk Human
After you have finished entering information, this form will be sent to your patient or their caregiver who will need to fill out their sections of the form as well. The patient assistance program provides medication at no cost to those who qualify. (v) coordinating the dispensing and delivery of medication; Novo nordisk patient assistance program hormone therapy po box.
Programa de asistencia con el producto Novoeight® (Antihemophilic
Patients who are approved for the pap may qualify to. Reserves the right to modify or cancel this program at any time without notice. (iii) identifying and/or determining eligibility under pap and other patient assistance resources; (iv) investigating and verifying my insurance benefits; Web the novo nordisk patient assistance program (pap) is based on our commitment to our patients.
Reserves The Right To Modify Or Cancel This Program At Any Time Without Notice.
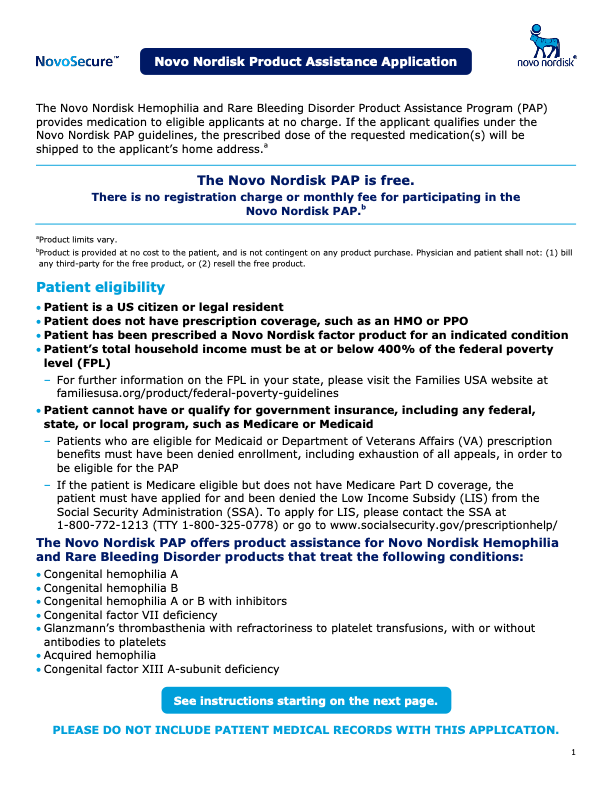
All information must be completed unless otherwise indicated. Web renewal the novo nordisk hormone therapy patient assistance program (pap) provides medication to eligible applicants at no charge. The patient assistance program provides medication at no cost to those who qualify. For uninsured patients, an approved application is valid for 12 months.
Web The Novo Nordisk Patient Assistance Program (Pap) Is Based On Our Commitment To Our Patients.
Patients who are approved for the pap may qualify to. Web novo nordisk patient assistance program (pap) available products victoza® (liraglutide) injection 1.2 mg 2 pen pack* victoza® (liraglutide) injection 1.8 mg 3 pen pack* ozempic® (semaglutide) injection pen that delivers doses of 0.25 mg or 0.5 mg (iv) investigating and verifying my insurance benefits; Novo nordisk patient assistance program hormone therapy po box 181640 louisville, ky 40261 novo nordisk inc.
After You Have Finished Entering Information, This Form Will Be Sent To Your Patient Or Their Caregiver Who Will Need To Fill Out Their Sections Of The Form As Well.
Patients can renew each year for as long as they qualify. (v) coordinating the dispensing and delivery of medication; (iii) identifying and/or determining eligibility under pap and other patient assistance resources; Web novo nordisk patient assistance program refill/reorder request form must be submitted directly by the hcp and must include a cover letter/hcp letterhead to clearly identify hcp as the sender.
Web Novo Nordisk Patient Assistance Program Application Instructions For Completing The Application Complete All Fields To Avoid Return Of Incomplete Application Make Sure The Application Is Signed By The Prescriber And Dated Remember To Include Disposable Pen Needles In The Order Information If Applicable
Web this personal information aids in administering pap by: