Novo Nordisk Refill Form
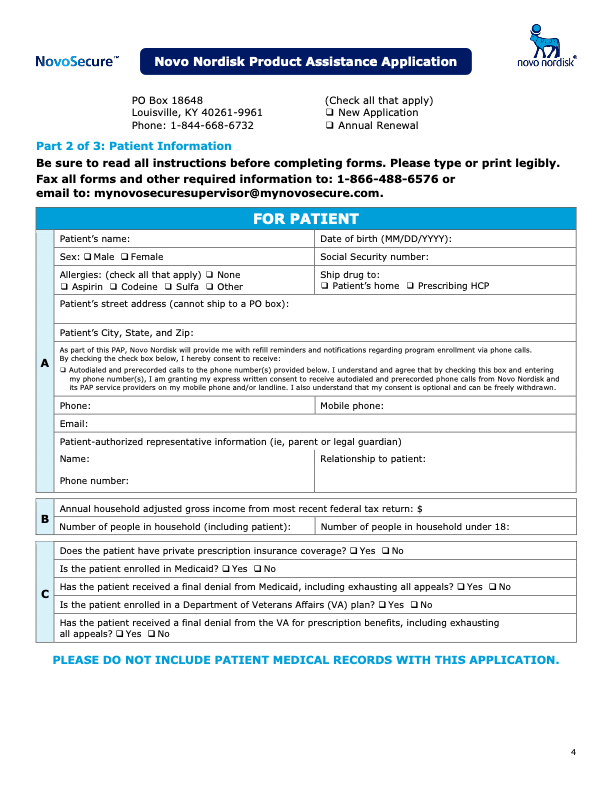
Novo Nordisk Refill Form - Save or instantly send your ready documents. Web service request form patient affordability and access support service request form wegovy™ (semaglutide) injection 2.4 mgsaxenda® (liraglutide) injection 3 mg program phone: Web novo nordisk patient assistance program refill/reorder request form must be submitted directly by the hcp and must include a cover letter/hcp letterhead to clearly identify hcp as the sender. Download share to download later. All new applicants will be automatically enrolled. For uninsured patients, an approved application is valid for 12 months. If you'd like to return to this page and download these materials later, just make sure you're logged in and then return through my toolbox. See how we can help go to the home page Patients can renew each year for as long as they qualify. Health care practitioner information section must be filled out completely patient information and eligibility section must be filled out completely
Patients are not required to use a third party who charges a fee to help with enrollment or refills. The medication will ship to the prescriber of an approved enrollee/applicant in accordance with currant program guidelines with minimal involvement on behalf of. Web service request form patient affordability and access support service request form wegovy™ (semaglutide) injection 2.4 mgsaxenda® (liraglutide) injection 3 mg program phone: All new applicants will be automatically enrolled. Health care practitioner information section must be filled out completely patient information and eligibility section must be filled out completely Easily fill out pdf blank, edit, and sign them. Patients can renew each year for as long as they qualify. Web new application refills (complete page 2 only) fax: All information must be completed unless otherwise indicated. For uninsured patients, an approved application is valid for 12 months.
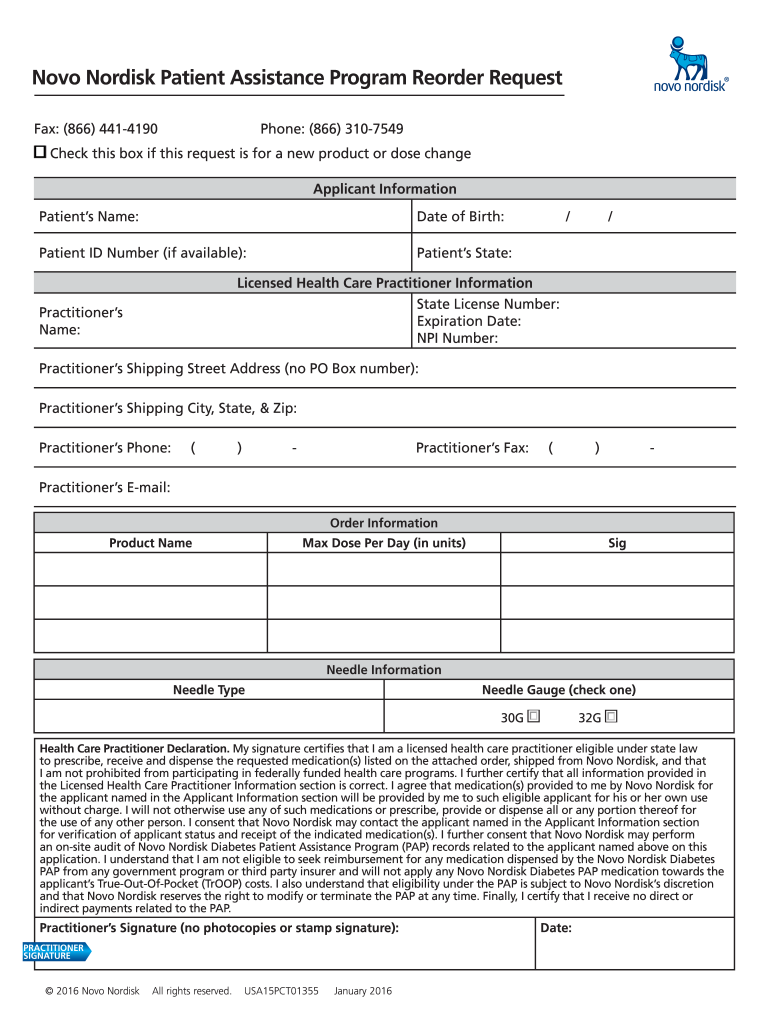
For uninsured patients, an approved application is valid for 12 months. Web novo nordisk patient assistance program refill/reorder request form must be submitted directly by the hcp and must include a cover letter/hcp letterhead to clearly identify hcp as the sender. Patients are not required to use a third party who charges a fee to help with enrollment or refills. Web new application refills (complete page 2 only) fax: All new applicants will be automatically enrolled. Form must be submitted directly by the hcp and must include a cover letter/. Easily fill out pdf blank, edit, and sign them. Web this form should be used by a health care practitioner to request a refill, to add a new medication, to request a change in medication or change in dosage for a current medication, or to update the health care practitioner information, such as address, suite number, etc. Download share to download later. See how we can help go to the home page

Novo Nordisk to boost pillform diabetic drugs with 1.8 billion deal
Web complete novo nordisk patient assistance refill form 2020 online with us legal forms. Easily fill out pdf blank, edit, and sign them. Health care practitioner information section must be filled out completely patient information and eligibility section must be filled out completely See how we can help go to the home page For uninsured patients, an approved application is.

Contact Novo Nordisk our local offices
See how we can help go to the home page Form must be submitted directly by the hcp and must include a cover letter/. Web novo nordisk patient assistance program refill/reorder request form must be submitted directly by the hcp and must include a cover letter/hcp letterhead to clearly identify hcp as the sender. Download share to download later. All.

Novo Nordisk A/S Forskningscenter E5+F5 RH ARKITEKTER AS Clinic
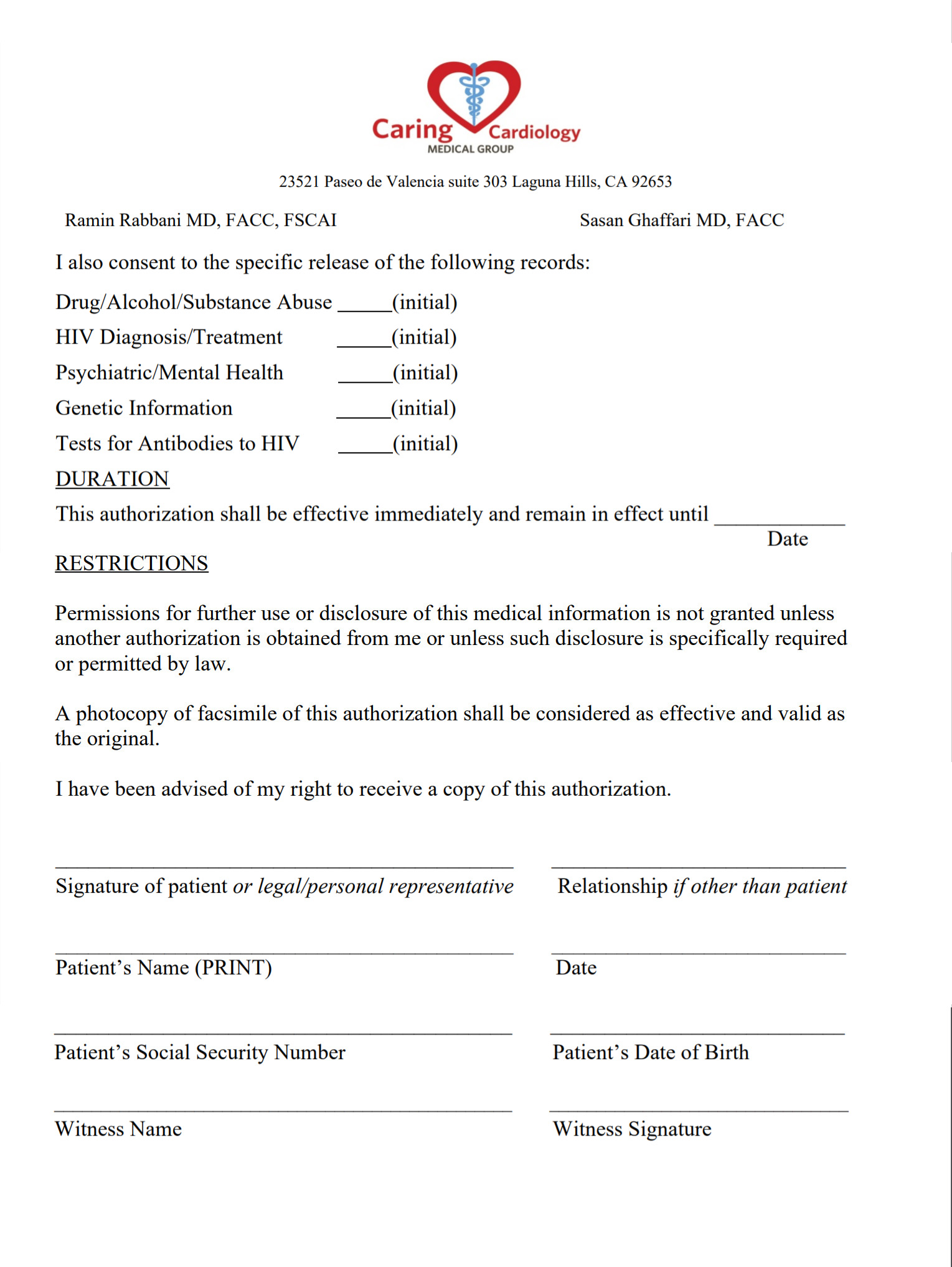
Download share to download later. Health care practitioner information section must be filled out completely patient information and eligibility section must be filled out completely Web download our authorization form and get started with novocare ® today. All information must be completed unless otherwise indicated. Web complete novo nordisk patient assistance refill form 2020 online with us legal forms.
Product Assistance Program Novoeight® (Antihemophilic Factor
Easily fill out pdf blank, edit, and sign them. Web this form should be used by a health care practitioner to request a refill, to add a new medication, to request a change in medication or change in dosage for a current medication, or to update the health care practitioner information, such as address, suite number, etc. The medication will.

With new FDA submission, Novo Nordisk aims to trumpet Tresiba's
Form must be submitted directly by the hcp and must include a cover letter/. The medication will ship to the prescriber of an approved enrollee/applicant in accordance with currant program guidelines with minimal involvement on behalf of. Web download our authorization form and get started with novocare ® today. See how we can help go to the home page Web.

novonordisk
Web new application refills (complete page 2 only) fax: Patients can renew each year for as long as they qualify. All new applicants will be automatically enrolled. Web for added convenience and at the direction of the prescriber, the novo nordisk pap now offers automatic refills for most medications. If you'd like to return to this page and download these.

List of Common Drugs and Medications to Treat Diabetes Escrow Refills
Patients can renew each year for as long as they qualify. Patients are not required to use a third party who charges a fee to help with enrollment or refills. Form must be submitted directly by the hcp and must include a cover letter/. Web this form should be used by a health care practitioner to request a refill, to.
Novo Nordisk Patient Assistance Refill Form 2020 Fill and Sign
Save or instantly send your ready documents. Health care practitioner information section must be filled out completely patient information and eligibility section must be filled out completely All new applicants will be automatically enrolled. All information must be completed unless otherwise indicated. For uninsured patients, an approved application is valid for 12 months.
Ozempic Patient Assistance Form Pdf
Web service request form patient affordability and access support service request form wegovy™ (semaglutide) injection 2.4 mgsaxenda® (liraglutide) injection 3 mg program phone: Web download our authorization form and get started with novocare ® today. Download share to download later. What would you like to do next? Web novo nordisk patient assistance program refill/reorder request form must be submitted directly.

Novo Nordisk 100 U/mL Novo Rapid Flexpen Inection, Packaging Type Box
The medication will ship to the prescriber of an approved enrollee/applicant in accordance with currant program guidelines with minimal involvement on behalf of. Download share to download later. What would you like to do next? Health care practitioner information section must be filled out completely patient information and eligibility section must be filled out completely Easily fill out pdf blank,.
Web This Form Should Be Used By A Health Care Practitioner To Request A Refill, To Add A New Medication, To Request A Change In Medication Or Change In Dosage For A Current Medication, Or To Update The Health Care Practitioner Information, Such As Address, Suite Number, Etc.
What would you like to do next? Patients can renew each year for as long as they qualify. All information must be completed unless otherwise indicated. Web download our authorization form and get started with novocare ® today.
Download Share To Download Later.
Web novo nordisk patient assistance program refill/reorder request form must be submitted directly by the hcp and must include a cover letter/hcp letterhead to clearly identify hcp as the sender. See how we can help go to the home page Web service request form patient affordability and access support service request form wegovy™ (semaglutide) injection 2.4 mgsaxenda® (liraglutide) injection 3 mg program phone: All new applicants will be automatically enrolled.
If You'd Like To Return To This Page And Download These Materials Later, Just Make Sure You're Logged In And Then Return Through My Toolbox.
Easily fill out pdf blank, edit, and sign them. For uninsured patients, an approved application is valid for 12 months. The medication will ship to the prescriber of an approved enrollee/applicant in accordance with currant program guidelines with minimal involvement on behalf of. Web for added convenience and at the direction of the prescriber, the novo nordisk pap now offers automatic refills for most medications.
Patients Are Not Required To Use A Third Party Who Charges A Fee To Help With Enrollment Or Refills.
Health care practitioner information section must be filled out completely patient information and eligibility section must be filled out completely Form must be submitted directly by the hcp and must include a cover letter/. Web new application refills (complete page 2 only) fax: Web complete novo nordisk patient assistance refill form 2020 online with us legal forms.