Us Rx Care Pa Form
Us Rx Care Pa Form - Web medication prior authorization form **please fax request to 888‐389‐9668 or mail to: Incomplete forms may delay processing. For prior authorization requests simply complete our short pa form and fax to us. Web reimbursement form if you are a member filing a paper claim for medication (s) purchased, please complete the direct member reimbursement form and fax it to the number. Incomplete forms may delay processing. Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.). Quality of care and service obsessed. Web request for prior authorization (pa) must include the member name, id#, dob, and drug name. Web request for prior authorization (pa) must include the member name, insurance, id#, date of birth, and drug name. Share your form with others
Web request for prior authorization (pa) must include the member name, insurance, id#, date of birth, and drug name. Share your form with others Incomplete forms will delay processing. Sign it in a few clicks draw your signature, type it, upload its image, or use your mobile device as a signature pad. Web us rx care will respond via fax or phone within 24 hours of all necessary information, except during weekends and holidays. Edit your us rx care prior authorization form online type text, add images, blackout confidential details, add comments, highlights and more. Contractual adherence to fiduciary standards on behalf of plan sponsors and plan enrollees. Quality of care and service obsessed. Our team is able to review and respond to most prior authorization requests within 24. For prior authorization requests simply complete our short pa form and fax to us.
Sign it in a few clicks draw your signature, type it, upload its image, or use your mobile device as a signature pad. Share your form with others Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.). Incomplete forms may delay processing. A request for prior authorization has been denied for lack of information received from the prescriber. There may be a drug specific fax form available** provider information member information prescriber name (print) member name (print) Web reimbursement form if you are a member filing a paper claim for medication (s) purchased, please complete the direct member reimbursement form and fax it to the number. Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.). Web medication prior authorization form **please fax request to 888‐389‐9668 or mail to: Incomplete forms will delay processing.

quest requisition form fill online printable fillable blank pdffiller
Web us rx care will respond via fax or phone within 24 hours of all necessary information, except during weekends and holidays. Incomplete forms may delay processing. There may be a drug specific fax form available** provider information member information prescriber name (print) member name (print) Web reimbursement form if you are a member filing a paper claim for medication.

Optum Rx Pa Form Fill and Sign Printable Template Online US Legal Forms
Sign it in a few clicks draw your signature, type it, upload its image, or use your mobile device as a signature pad. Our team is able to review and respond to most prior authorization requests within 24 hours if not the same day. A request for prior authorization has been denied for lack of information received from the prescriber..
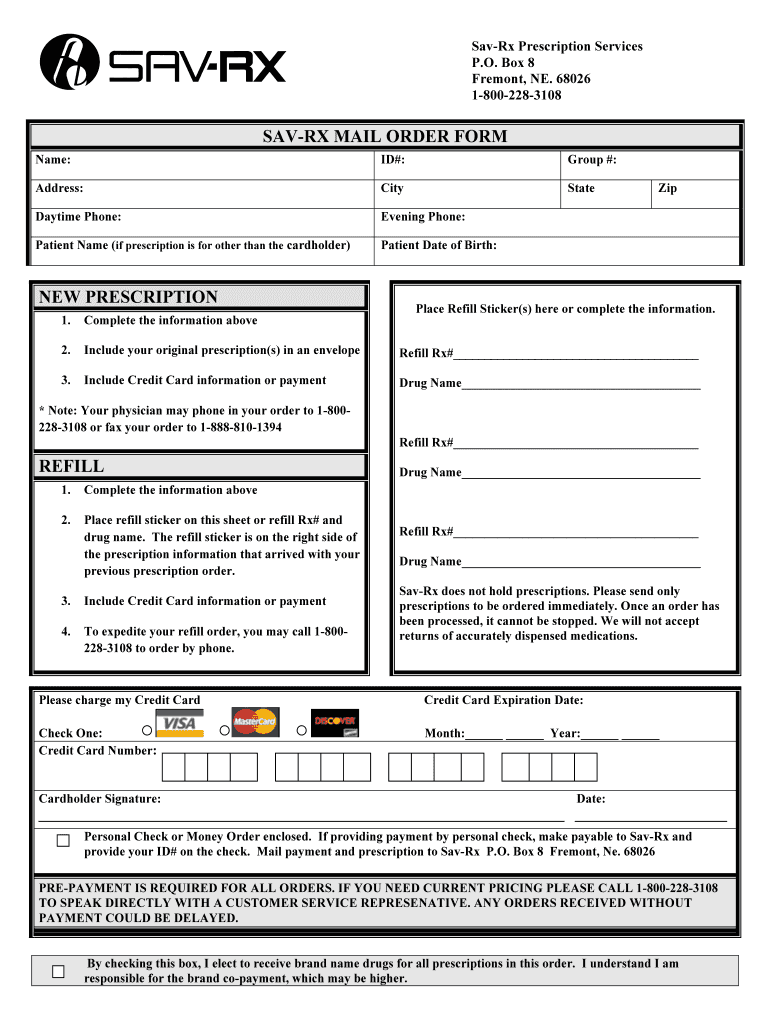
Savrx Pa Form Fill Out and Sign Printable PDF Template signNow
Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.). Incomplete forms will delay processing. A request for prior authorization has been denied for lack of information received from the prescriber. Our team is able to review and respond to most prior authorization requests within 24. Share your form with others

Request for prior authorization (pa) must include member name, id#, dob and drug name. Our team is able to review and respond to most prior authorization requests within 24. Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.). Web request for prior authorization (pa) must include the member name, id#, dob, and.

USRx Care Fiduciary Pharmacy Benefit Services YouTube
Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.). Our team is able to review and respond to most prior authorization requests within 24. Incomplete forms may delay processing. Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.). Incomplete forms will delay processing.
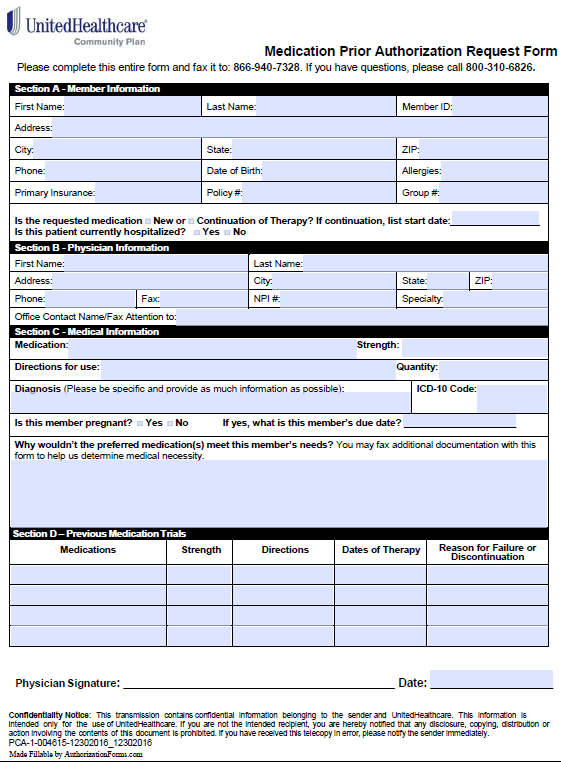
Free United Healthcare Prior Prescription (Rx) Authorization Form PDF
Our team is able to review and respond to most prior authorization requests within 24. Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.). Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.). Incomplete forms may delay processing. Web reimbursement form if you are.

USRx Care
There may be a drug specific fax form available** provider information member information prescriber name (print) member name (print) Edit your us rx care prior authorization form online type text, add images, blackout confidential details, add comments, highlights and more. Web reimbursement form if you are a member filing a paper claim for medication (s) purchased, please complete the direct.

Home
There may be a drug specific fax form available** provider information member information prescriber name (print) member name (print) For prior authorization requests simply complete our short pa form and fax to us. Web request for prior authorization (pa) must include the member name, id#, dob, and drug name. Incomplete forms may delay processing. Incomplete forms will delay processing.

Reviews Pharmacy That Lacks Feedback RxStars RxStars
Incomplete forms may delay processing. Incomplete forms may delay processing. There may be a drug specific fax form available** provider information member information prescriber name (print) member name (print) Web reimbursement form if you are a member filing a paper claim for medication (s) purchased, please complete the direct member reimbursement form and fax it to the number. Our team.

RightMed Save on your medications today!
Web request for prior authorization (pa) must include the member name, insurance, id#, date of birth, and drug name. Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.). Web us rx care will respond via fax or phone within 24 hours of all necessary information, except during weekends and holidays. Web medication.
Web Medication Prior Authorization Form **Please Fax Request To 888‐389‐9668 Or Mail To:
Share your form with others Our team is able to review and respond to most prior authorization requests within 24 hours if not the same day. Web us rx care will respond via fax or phone within 24 hours of all necessary information, except during weekends and holidays. Please include lab reports with request when appropriate (e.g., c&s, hga1c, serum cr, cd4, h&h, wbc, etc.).
Please Include Lab Reports With Request When Appropriate (E.g., C&S, Hga1C, Serum Cr, Cd4, H&H, Wbc, Etc.).
A request for prior authorization has been denied for lack of information received from the prescriber. Edit your us rx care prior authorization form online type text, add images, blackout confidential details, add comments, highlights and more. Our team is able to review and respond to most prior authorization requests within 24. Sign it in a few clicks draw your signature, type it, upload its image, or use your mobile device as a signature pad.
Contractual Adherence To Fiduciary Standards On Behalf Of Plan Sponsors And Plan Enrollees.
Web request for prior authorization (pa) must include the member name, insurance, id#, date of birth, and drug name. There may be a drug specific fax form available** provider information member information prescriber name (print) member name (print) Incomplete forms will delay processing. Incomplete forms may delay processing.
Quality Of Care And Service Obsessed.
Web request for prior authorization (pa) must include the member name, id#, dob, and drug name. Request for prior authorization (pa) must include member name, id#, dob and drug name. Web reimbursement form if you are a member filing a paper claim for medication (s) purchased, please complete the direct member reimbursement form and fax it to the number. For prior authorization requests simply complete our short pa form and fax to us.