Wellcare Appeal Form Pdf
Wellcare Appeal Form Pdf - Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. It’s easy to ask for an. Web member appeal form complete and mail or fax to: Save or instantly send your ready documents. Save or instantly send your ready. Expedited appeal requests can be. Detox and substance abuse service request. Easily fill out pdf blank, edit, and sign them. All fields are required information:
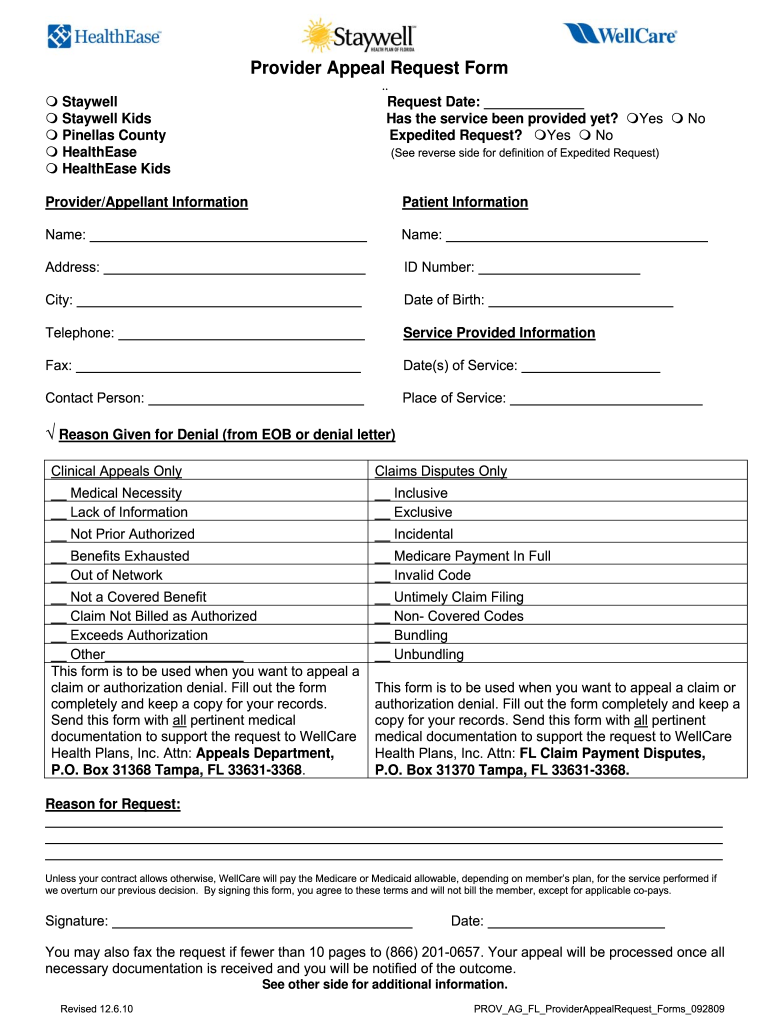
Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Web because <<strong>wellcare</strong>> health plans denied your request for coverage of (or payment for) a prescription drug, you have the right to an appeal. You can now quickly request an appeal for your drug coverage through the. Web wellcare appeal form pdf. Web with dochub, making changes to your paperwork takes only a few simple clicks. Web disputes, reconsiderations and grievances. Web request to wellcare health plans, inc., attn: Providers may file a verbal or written complaint with the missouri care complaints and appeals department. Web provider resources prior authorization request form (pdf) inpatient fax cover letter (pdf) medication appeal request form (pdf) medicaid drug coverage request. Web as a member of health net you have the right to file an appeal for any denials related to medical services (part c) or prescription drug (part b) coverage.
We have redesigned our website. Web because <<strong>wellcare</strong>> health plans denied your request for coverage of (or payment for) a prescription drug, you have the right to an appeal. Detox and substance abuse service request. Web request for medicare prescription drug coverage determination. Get everything done in minutes. Follow these quick steps to edit the pdf wellcare appeal form online free of charge: Easily fill out pdf blank, edit, and sign them. Web provider resources prior authorization request form (pdf) inpatient fax cover letter (pdf) medication appeal request form (pdf) medicaid drug coverage request. Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Web disputes, reconsiderations and grievances.

OvertheCounter (OTC) Catalog WellCare Fill and Sign Printable
You can now quickly request an appeal for your drug coverage through the. Easily fill out pdf blank, edit, and sign them. Web as a member of health net you have the right to file an appeal for any denials related to medical services (part c) or prescription drug (part b) coverage. Easily fill out pdf blank, edit, and sign.
Wellcare Behavioral Health Service Request Form Fill Out and Sign
Web request for medicare prescription drug coverage determination. It’s easy to ask for an. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Complaints should be addressed to: We have redesigned our website.
United Healthcare Provider Claim Appeal Form baturinadesigns
Expedited appeal requests can be. Follow these quick steps to edit the pdf wellcare appeal form online free of charge: Web wellcare appeal form pdf. Web go to login register for an account welcome, pdp member! Save or instantly send your ready documents.

Appeal Form
Detox and substance abuse service request. You can use one of the determination forms to complete a medicare drug coverage request:. Web because <<strong>wellcare</strong>> health plans denied your request for coverage of (or payment for) a prescription drug, you have the right to an appeal. All fields are required information: Web a repository of medicare forms and documents for wellcare.
Free Wellcare Prior Prescription (Rx) Authorization Form PDF
Easily fill out pdf blank, edit, and sign them. The means you may ask us to review. Web with dochub, making changes to your paperwork takes only a few simple clicks. Wellcare| appeals & grievances/medicare operations. Web requesting an appeal (redetermination) if you disagree with medicare’s coverage or payment decision.
Fillable Outpatient Notification /authorization Request Wellcare
Web as a member of health net you have the right to file an appeal for any denials related to medical services (part c) or prescription drug (part b) coverage. Web requesting an appeal (redetermination) if you disagree with medicare’s coverage or payment decision. The means you may ask us to review. You can now quickly request an appeal for.
Recredentialing Application For Wellcare Fill Out and Sign Printable
Web wellcare appeal form pdf. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web because <<strong>wellcare</strong>> health plans denied your request for coverage of (or payment for) a prescription drug, you have the right to an appeal. Complaints should be addressed to: Web request for redetermination of medicare prescription.
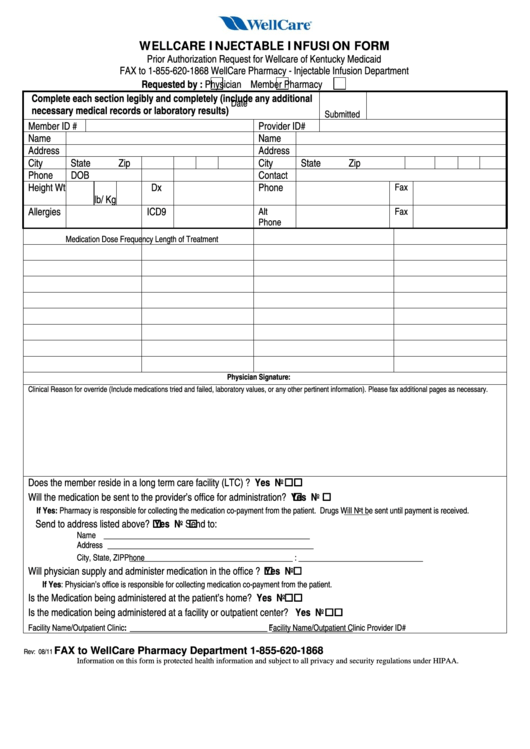
Fillable Wellcare Injectable Infusion Form Prior Authorization
Easily fill out pdf blank, edit, and sign them. You can use one of the determination forms to complete a medicare drug coverage request:. Web go to login register for an account welcome, pdp member! The means you may ask us to review. Save or instantly send your ready documents.
Wellcare Appeal Form Pdf Fill Online, Printable, Fillable, Blank
All fields are required information: Complaints should be addressed to: Wellcare| appeals & grievances/medicare operations. Web disputes, reconsiderations and grievances. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor.
Free Wellcare Prior Prescription (Rx) Authorization Form PDF
Web request to wellcare health plans, inc., attn: All fields are required information: Or visit our website at www.wellcarenc.com if you need help with your appeal request. We have redesigned our website. Expedited appeal requests can be.
Web As A Member Of Health Net You Have The Right To File An Appeal For Any Denials Related To Medical Services (Part C) Or Prescription Drug (Part B) Coverage.
Web because <<strong>wellcare</strong>> health plans denied your request for coverage of (or payment for) a prescription drug, you have the right to an appeal. Save or instantly send your ready documents. It’s easy to ask for an. Web requesting an appeal (redetermination) if you disagree with medicare’s coverage or payment decision.
You Can Now Quickly Request An Appeal For Your Drug Coverage Through The.
The means you may ask us to review. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Easily fill out pdf blank, edit, and sign them. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process.
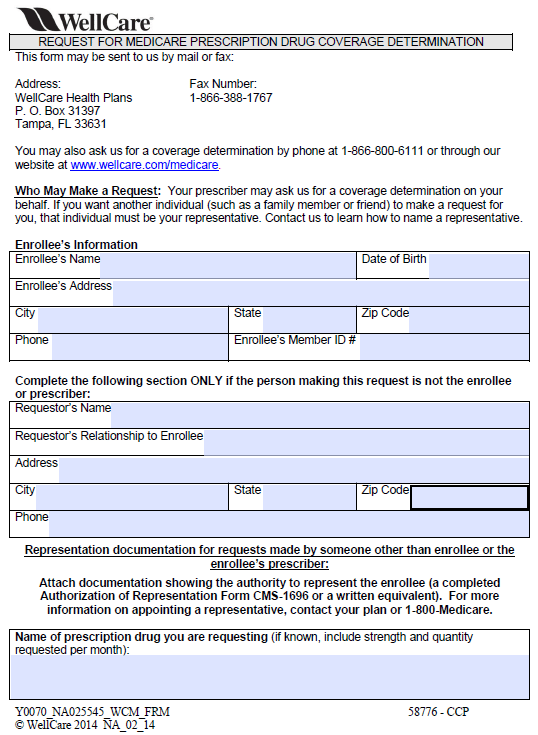
Web Request For Medicare Prescription Drug Coverage Determination.
Or visit our website at www.wellcarenc.com if you need help with your appeal request. Providers may file a verbal or written complaint with the missouri care complaints and appeals department. Easily fill out pdf blank, edit, and sign them. You can use one of the determination forms to complete a medicare drug coverage request:.
Web Request For Redetermination Of Medicare Prescription Drug Denial (Appeal) (Pdf) This Form May Be Sent To Us By Mail Or Fax:
Web member appeal form complete and mail or fax to: Web wellcare appeal form pdf. Web go to login register for an account welcome, pdp member! Complaints should be addressed to: