Molina Direct Referral Form
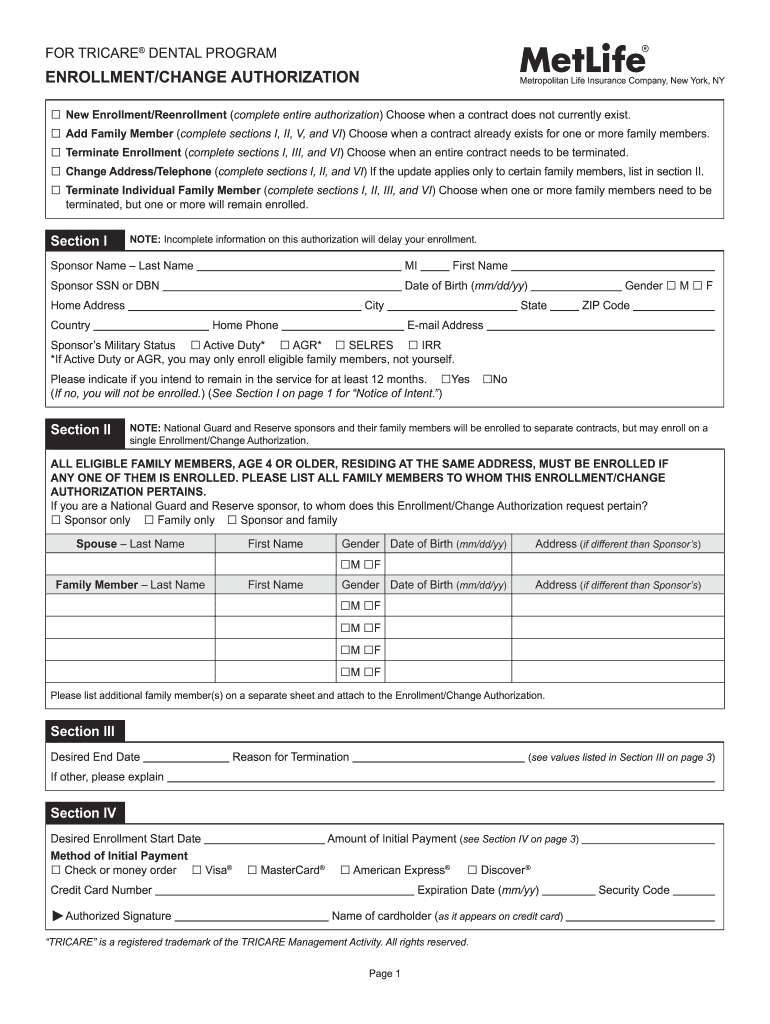
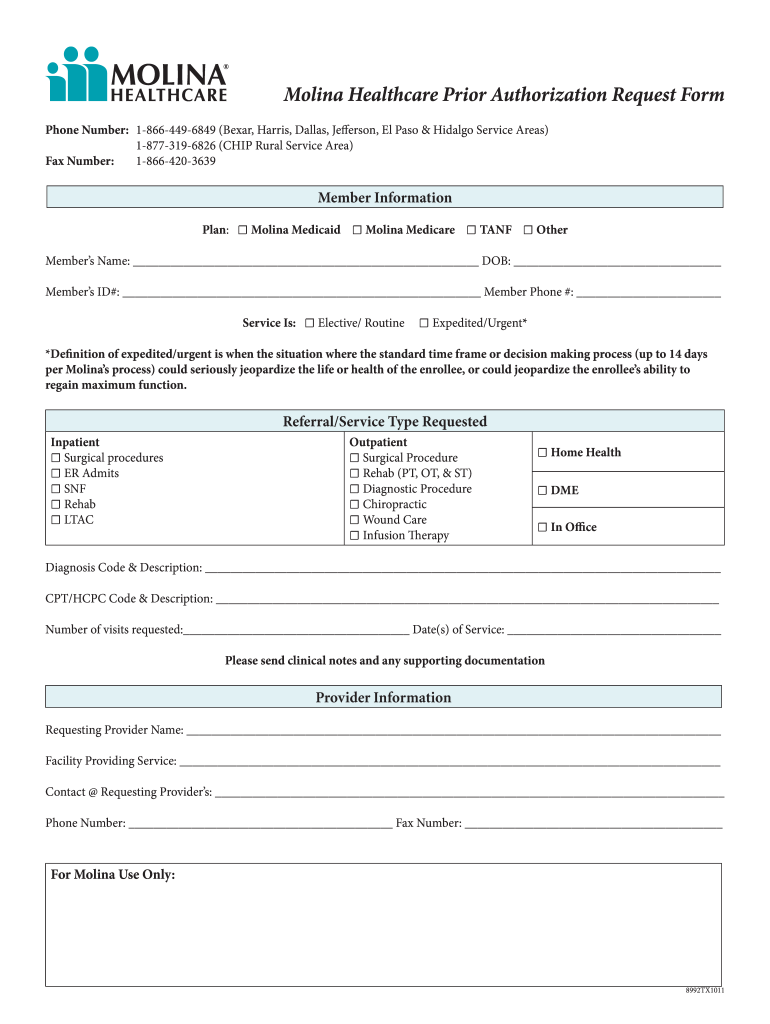
Molina Direct Referral Form - All patients return to their referring physician, as the physician is the hub of medical management. Web prolia® (denosumab) prior authorization request form; Member grievance and appeals request form ( english | spanish) medical release form ( english | spanish) authorization for the use and disclosure of. Web use our referral form to expedite your patient’s appointment. A referral is required to participate in evaluation and. Behavioral health therapy prior authorization form (autism). Web direct referral form fax to: Please read and fill out the entire form. This form must be completely filled out in order to process your claim(s). Web direct referrals are only valid to a molina healthcare contracted specialist please note:
Provider authorization guide/service request form (effective: Web direct referral form fax to: Web molina healthcare of washington, inc. Protopic ® (tacrolimus) prior authorization request form; A referral is required to participate in evaluation and. Behavioral health prior authorization form. All patients return to their referring physician, as the physician is the hub of medical management. Web to better support our providers and members, we created a care management referral form that providers can complete and fax directly to us when providers identify a member who. Web critical incident referral template (medicaid only) ohio urine drug screen prior authorization (pa) request form pac provider intake form Electronic data interchange (edi) quality of care incident.
A referral is required to participate in evaluation and. Behavioral health prior authorization form. Web use our referral form to expedite your patient’s appointment. Web molina healthcare of washington, inc. Web direct referral to specialist* validate eligibility prior to referral. Electronic data interchange (edi) quality of care incident. Critical incident form email comped et l form o:t mhw.critical_incidents@molinahealthcare.com type of incident (required by. Web support coordination (case management) is intended to assist individuals in gaining access to needed supports and services, regardless if these are natural supports,. We are able to meet your requested appointment timeframe 97 % of the time. Web direct member reimbursement form directions:
Direct Referral Corinne Evans Physiotherapy Clinic Tralee
Specialists are required to submit reports. Provider authorization guide/service request form (effective: Behavioral health prior authorization form. Protopic ® (tacrolimus) prior authorization request form; Behavioral health therapy prior authorization form (autism).

Medical Referral form Template Fresh 6 Counselling Referral for
All patients return to their referring physician, as the physician is the hub of medical management. Behavioral health prior authorization form. Electronic data interchange (edi) quality of care incident. Web claims provider dispute resolution request form prior authorizations behavioral health prior authorization form behavioral health therapy prior authorization form (autism). Member grievance and appeals request form ( english | spanish).
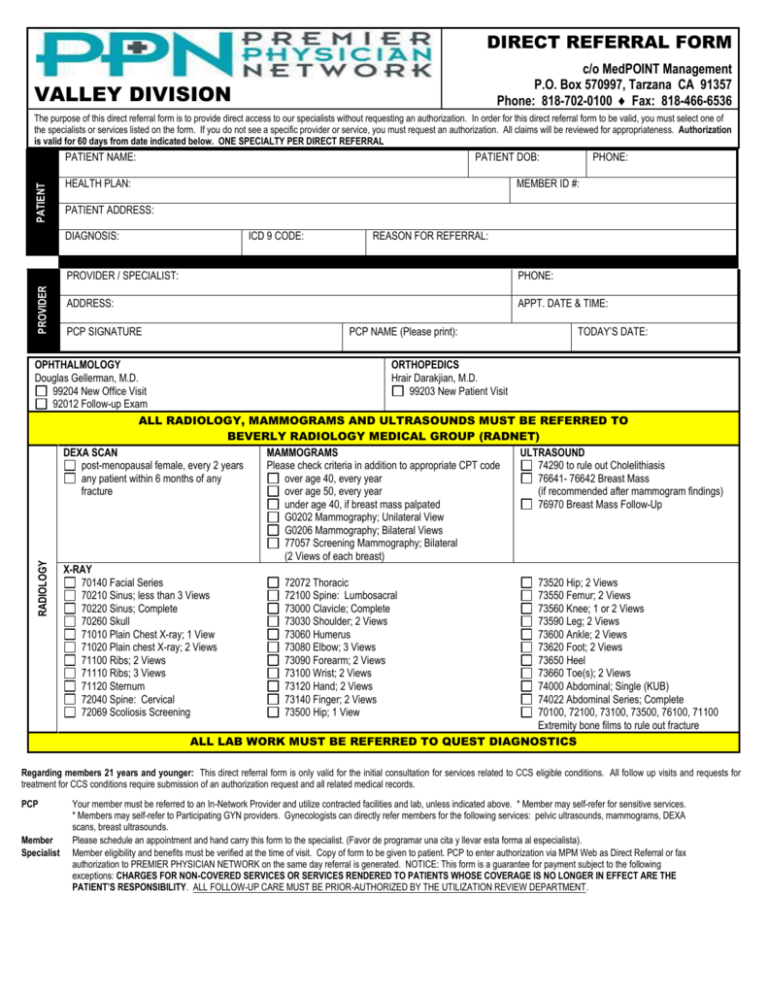
Metlife Disenrollment Met Form Fill Out and Sign Printable PDF
Please read and fill out the entire form. Web critical incident referral template (medicaid only) ohio urine drug screen prior authorization (pa) request form pac provider intake form Psychotropic agents for children age 0 to 5;. Provider authorization guide/service request form (effective: A referral is required to participate in evaluation and.
Molina Prior Authorization Form 2021 Fill Online, Printable, Fillable
Behavioral health therapy prior authorization form (autism). Web support coordination (case management) is intended to assist individuals in gaining access to needed supports and services, regardless if these are natural supports,. Psychotropic agents for children age 0 to 5;. Web to better support our providers and members, we created a care management referral form that providers can complete and fax.

Molina Healthcare Prescription Drug Prior Authorization Request Form
1/1/2020) 2020 codification document (effective 4/1/2020)). Web use our referral form to expedite your patient’s appointment. Psychotropic agents for children age 0 to 5;. We are able to meet your requested appointment timeframe 97 % of the time. Critical incident form email comped et l form o:t mhw.critical_incidents@molinahealthcare.com type of incident (required by.

Customer Referral HF Direct
Member grievance and appeals request form ( english | spanish) medical release form ( english | spanish) authorization for the use and disclosure of. Web molina healthcare of washington, inc. We are able to meet your requested appointment timeframe 97 % of the time. Web prolia® (denosumab) prior authorization request form; Web direct member reimbursement form directions:
PPN Valley Direct Referral Form 2015
This form must be completely filled out in order to process your claim(s). Web direct referrals are only valid to a molina healthcare contracted specialist please note: Electronic data interchange (edi) quality of care incident. If member is assigned to an ipa/medical group you must refer to the ipa's policy for referral. Web critical incident referral template (medicaid only) ohio.

Optumrx New Form Fill Online, Printable, Fillable, Blank pdfFiller
Web direct referral form fax to: Member grievance and appeals request form ( english | spanish) medical release form ( english | spanish) authorization for the use and disclosure of. Behavioral health prior authorization form. We are able to meet your requested appointment timeframe 97 % of the time. Please read and fill out the entire form.

Customer Referral HF Direct
Web direct member reimbursement form directions: This form must be completely filled out in order to process your claim(s). Web use our referral form to expedite your patient’s appointment. Web direct referral to specialist* validate eligibility prior to referral. Please read and fill out the entire form.
Molina Authorization Form Fill Online, Printable, Fillable, Blank
Web direct referral form fax to: Web direct member reimbursement form directions: Web support coordination (case management) is intended to assist individuals in gaining access to needed supports and services, regardless if these are natural supports,. 1/1/2020) 2020 codification document (effective 4/1/2020)). Electronic data interchange (edi) quality of care incident.
Web Direct Referral To Specialist* Validate Eligibility Prior To Referral.
Provider authorization guide/service request form (effective: A referral is required to participate in evaluation and. This form must be completely filled out in order to process your claim(s). Web to better support our providers and members, we created a care management referral form that providers can complete and fax directly to us when providers identify a member who.
Web Therapies, Please Direct Prior Authorization Requests To Novologix Via The Molina Provider Portal.
Behavioral health therapy prior authorization form (autism). Web molina healthcare of washington, inc. Electronic data interchange (edi) quality of care incident. Psychotropic agents for children age 0 to 5;.
Member Grievance And Appeals Request Form ( English | Spanish) Medical Release Form ( English | Spanish) Authorization For The Use And Disclosure Of.
Web prolia® (denosumab) prior authorization request form; Behavioral health prior authorization form. Web direct member reimbursement form directions: Please read and fill out the entire form.
Web Direct Referrals Are Only Valid To A Molina Healthcare Contracted Specialist Please Note:
Web claims provider dispute resolution request form prior authorizations behavioral health prior authorization form behavioral health therapy prior authorization form (autism). Critical incident form email comped et l form o:t mhw.critical_incidents@molinahealthcare.com type of incident (required by. Web critical incident referral template (medicaid only) ohio urine drug screen prior authorization (pa) request form pac provider intake form 1/1/2020) 2020 codification document (effective 4/1/2020)).